Harbor:Operations manual: Difference between revisions
| Line 234: | Line 234: | ||
===21.5 Medications in Triage: Standardized Procedure=== | ===21.5 Medications in Triage: Standardized Procedure=== | ||
* Administration of medications in triage (MIT) is to provide timely treatment for patients arriving to the ED in pain, with fever, with dyspepsia, or N/V. Patients in pain should be offered oral analgesia at the time of triage/assessment and reassessment. | |||
* DEM Triage RN's have received additional training in giving medications in triage and may administer medications (Acetaminophen, Ibuprofen, Aluminum hydroxide and Magnesium hydroxide antacid [Mag-Al Plus], or Ondansetron) to patients when indicated by the specific requirements of this procedure unless contra-indicated. | |||
** PAIN: All patients who arrive to the ED Triage area will have their level of pain assessed and documented in the EMR. The pain scales used are FLACC, Numeric, and Faces, depending upon the age of the patient. Dosages for fever and/or pain shall be as follows: | |||
*** Child < 12 years of age – Acetaminophen 15mg/kg PO x 1 (max 650 mg) | |||
*** Child ≥ 12 years of age – Acetaminophen 15mg/kg PO x 1 (max 650 mg) | |||
*** Child > 6 months of age – Ibuprofen 10mg/kg PO x 1 (max 400 mg) | |||
*** Adult – Acetaminophen 650 mg PO x 1 | |||
*** Adult – Ibuprofen 400 mg PO x 1 | |||
** FEVER: All patients who present to the ED Triage area will have their temperatures taken and documented in the electronic medical record. All patients who present with a temperature > 100.4º F (38º C) [can be axillary, rectal, or oral temperature] shall be offered acetaminophen or ibuprofen. If a previous antipyretic has been given (either at home or in triage), an alternate antipyretic will be given if temperature >100.4º F (38º C). Rectal temperatures must be obtained for all of the following pediatric patients: Infants less than 2 months old, Children less than 2 years old with the exception of children presenting with minor trauma, & Active seizure patients up to 3 years old | |||
** DYSPEPSIA: Patients with a history of heartburn, gastritis, GERD, or dyspepsia or who complain of epigastric pain consistent with those conditions (e.g. burning epigastric pain that is relieved by food or antacids and worsened by spicy foods) shall be offered aluminum hydroxide and magnesium hydroxide antacid (Mag-Al Plus). Dosages shall be as follows: | |||
*** Child 3 – 11 years of age – 0.5 ml/kg (maximum 30ml) | |||
*** Child ≥ 12 years of age and Adult – 30ml PO | |||
** NAUSEA: Patients with a complaint of nausea or vomiting will be offered Ondansetron orally. Dosages shall be as follows: Ondansetron ODT (oral disintegrating tab), oral solution, or IV form orally | |||
*** Child 6 months to 3 years of age – 2mg PO | |||
*** Child 4 – 11 years of age – 4mg PO | |||
*** Child 12 years of age to Adult – 4mg PO | |||
* Reassessment and Repeat Dosing | |||
** Assessment of the patient’s symptoms (pain, fever, gastritis symptoms, nausea and/or vomiting) should be reassessed within 1 hours of the medication given in triage. | |||
** Patients who after reassessment of pain (within one hour of receiving the 1st dose of acetaminophen or ibuprofen) continue to complain of pain and desire further analgesic treatment will then be offered acetaminophen or ibuprofen alternating from the previous medication administration. | |||
**Patients who continue to complain of pain and/or fever may have a repeat dose of acetaminophen 4 hours after the initial dose, and/or a repeat dose of ibuprofen 6 hours after the initial dose. | |||
**Patients who continue to complain of dyspepsia may have a repeat dose of aluminum hydroxide and magnesium hydroxide antacid (Mag-Al Plus) 6 hours after the initial dose. | |||
* A nurse practitioner or physician provider will be notified of any patient that: | |||
** The triage nurse assesses to require more analgesia than oral acetaminophen or ibuprofen or aluminum hydroxide and magnesium hydroxide antacid (Mag-Al Plus) can provide | |||
** Develops any signs and/or symptoms of adverse reaction to acetaminophen, ibuprofen, aluminum hydroxide and magnesium hydroxide antacid (Mag-Al Plus), or ondansetron | |||
**Any medication error that occurs shall be brought to the attention of the Attending overseeing the patient and the nurse who administered the medication. The patient and/or caretaker will be informed of the error. Standard procedures will be followed, as is the Department’s policy for other medication errors. | |||
Approved November 2015, Chappell 2/22/16 | |||
==See Also== | ==See Also== | ||
Revision as of 00:04, 23 February 2016
ADULT ACUTE ED
ECG Screening by Providers
- CP patients from Triage get ECG in RME 1.
- ECG tech hands ECG to Provider.
- Who can sign ECG's electronically:
- ED Attendings and PGY-4's can sign electronically ("No STEMI Activation")
- NP's can sign electronically in ORCHID only for ECGs that say “Normal Sinus Rhythm.”
- For ECGs that say anything else, if the ECG is already uploaded into ORCHID, the NP can call an ED attending (x23202 or 23206) for the electronic ECG screen
- If the ECG is not yet uploaded, the NP need to hand to an ED attending who will perform the electronic ECG screen.
- PGY 1-3's can only visually review the ECG but then must hand off to or call an Attending or R4 to sign electronically
Chappell 4/2017
iSTAT Tests
EG7: Na, K, Ca, Hgb/Hct, Blood Gas (pH, pCO2, pO2, TCO2, HCO3, base excess, sO2)
CG4: Lactate, Blood Gas (pH, pCO2, pO2, TCO2, HCO3, base excess, sO2)
Admitting a Patient
We have admitting privileges to all hospital services. Once a patient is admitted by us, the service has two hours to write admitting orders or the ED will do it for them. We should hold services to the two-hour time limit as closely as possible in order to expedite ED flow.
If you are not sure if a patient needs to be admitted, you may always consult the service instead. Please make sure that the residents make it clear to the service that they are either admitting or consult on a patient.
When admitting patients, please follow the "Admission and Consultation Guidelines" as closely as possible to determine which service to admit to. If not listed, emergency department determines the admitting service.
The admission process steps below should be followed in strict order to avoid admission errors.
- Place an 'Interqual Request' to begin Utilization Review (UR) process.
- Resident or nurse practitioner in RME must discuss the case with the attending, who must agree with the admission.
- The attending must write a note in the orchid specifying the following three things:
- Service to admit to (if to the general surgical service, It should be listed as "Acute-Care Surgery" for the admitting service, even though the trauma service officially does all of our consults in the emergency department. Observation patients are not technically admitted, for these put "OBS", and for CORE patients put "CORE".
- Reason for admission: if the service itself made the decision to admit, then put "at request of ______ (Service). Otherwise note the brief medical indication for admission. "Placement" may be used as a reason to place the patient observation service; we do not admit placement patients to the hospital. You may put a more detailed justification in your attending note.
- Level of care (Ward, PCU, ICU, Tele)
- Once the admission note is placed by the attending, then the resident may contact the service to inform them of the admission. At this time the service can discuss the admission with emergency physician if they feel the admission is not justified or the patient should be admitted to another service. It is especially helpful if they have other information about the patient which may be important for a disposition decision. The final decision rests with emergency physicians, but if there is significant disagreement the ED attending should be involved in the discussion.
- Once the service has been informed, the ED resident should place the order "Request for Admit", which defines the time of admission decision. From this time the admitting service has two hours to disposition the patient. They may discharge the patient, write admitting orders for the patient, or transfer the patient to another service. ED department physicians should not be involved in these transfers; once the patient has been transferred to a new service, that service must contact the ED at which time a new two-hour period is established. The admitting service is responsible for the care of the patient once the "Request for Inpatient Bed" order is placed
- if the admitting service does not write admitting orders within the two-hour timeframe, the ED resident should contact the admitting service, or if unable, have made a reasonable effort to contact it makes service to inform them that the ED is going to write admitting orders. The ED resident then should proceed to write a brief admitting order set. ED attendings need to encourage the writing of admission order sets by the ED as soon after the two-hour time limit is up in order to expedite flow.
Admitting a patient
OBS/CORE
Admit Guidelines
- Who goes to what service (Admission and consultation guidelines)
- Post-admission management/Orders on Admitted Patients
Admission and Consultation Rules
The following guidelines for specific medical disorders are intended to expedite care of ED patients. They have been reviewed and agreed upon by all Departments and Divisions that provide consultation to the Adult ED.
The detailed guidelines can be found in HUMC Policies 312 File:HUMC Policy 312.pdf and 370 File:HUMC Policy 370.pdf (Official Feb 2020). Any new agreements are so annotated below.
Admission Decisions
- The ED Attending will determine the need for admission for all ED patients (AED, RME, PED) with input from consulting services
- The ED Attending will determine appropriateness for OBS/CORE with input from UR
- The ED attending has admitting privileges to all inpatient services; for cases with no specific guidelines, the ED Attending will use their best professional judgment in determining the admitting service
- The ED Attending should document the rationale for admission, admitting service, and required level of care
- A collaborative discussion should be had with the admitting service
- After discussion with the admitting service, the ED provider will place the admission order which transfers care to the admitting service (unless there is a medical emergency)
- If an admitting service attending feels the patient would be best cared for on another inpatient service, the admitting attending should speak to the attending of that service and a final decision should be accomplished and reported back to the ED attending within 30 minutes; if this does not occur, escalate to the associate/CMO who will make the decision
- If there is disagreement about a admitting service, the ADMITTING ATTENDING NEEDS TO CALL THE ALTERNATE/MORE APPROPRIATE ADMITTING SERVICE ATTENDING
- If an admitting service attending feels the patient would be best cared for on another inpatient service, the admitting attending should speak to the attending of that service and a final decision should be accomplished and reported back to the ED attending within 30 minutes; if this does not occur, escalate to the associate/CMO who will make the decision
- If the admitting service has not evaluated the patient and placed orders within 2 hours of the admission, the ED should place abbreviated admission orders ("holding orders" - activity, vitals, oxygen, IV)
- Patients <18 will be admitted to Pediatrics; ages 18-20 will be admitted to Pediatrics at the discretion and capacity of the Peds service
Consults
- Always check Medhub for the most current schedule
- If no one is listed, please call ED AOD to escalate to Drs. Gutierrez & Harrington
- Consult via Orchid as soon as you know the service is needed to expedite patient throughput
- Service transition time is generally 7am (from night team to the following day team)
- Agreed by:
- Hand Call @ 7am (6/5/23): Plastics (Dr. Do), Ortho (Dr. Gold)
- Face Call @ 7am (6/12/23): Plastics (Dr. Do), OMFS (Dr. Crum), ENT (Dr. Kedeshian), Dr. de Virgilio (Surgery Chair)
- Agreed by:
Complicating Medical Conditions (CMC)
- One or more active acute medical conditions that the non-IM/FM service does not usually manage AND is likely to require ongoing management or active monitoring during the hospitalization; the decision of what constitutes a CMC is made by the ED Attending
- Any discussion for most appropriate admitting service given a CMC will occur at the attending level (inpatient service & ED); elevation to division chief/department chair, then associate/CMO (Dr. Stein/Dr. Mahajan); chief residents cannot replace an attending for this discussion
- Service specific, so it might vary by services
- Consideration: Simply having stable co-morbidities that require continuation of home medications and therapies does NOT constitute a reason to deviate from the admission guidelines
- Consideration: Significant co-morbidities that separately would require admission to a medicine service, consider admitting that patient to medicine with the surgical or specialty service on consult
- If there is disagreement about a CMC, the ADMITTING ATTENDING NEEDS TO CALL THE ED ATTENDING
- Service specific, so it might vary by services
- Residents cannot overrule admission decisions made by the ED attending
- Residents cannot discharge a patient from the ED who has been admitted to their service without an explicit discussion and agreement from their attending
- If an admitting service attending feels the patient would best be cared for on another inpatient service, the admitting attending should speak with the attending of that service. A final decision between the two inpatient service attendings about which admitting service is most appropriate should be accomplished within 30 minutes and reported back to the ED attending.
- Assisting services for specific CMCs
- Primary surgical admission requiring ICU care will be admitted to the trauma/surgical ICU
- C-team can be consulted for CHF as a complicating medical condition
- Nephrology can be consulted to assist with HTN as a complicating medical condition
- Geriatrics may be consulted 24/7 and is available to assist in the care of patients greater than 65 years old (will go as low as 60 for ortho patients)
- Endocrine: may be consulted to assist with blood sugar management
- Nephrology: may be consulted to assist with blood pressure control; if the patient needs cardiac clearance as well, cardiology can perform this function and help manage hypertension
- Pre-operative Clearance: If >65, consult geriatrics; otherwise, third-call can assist in providing this service
Aortic Aneurysms
- Aortic Aneurysms & Dissections
- Thoracic (Type A or B) - admit to trauma surgery (or CTS if immediately available)
- Abdominal Aneurysm
- Expanding or ruptured to trauma (or vascular if immediately available)
- Stable aneurysms can be admitted to other services based on reason for admission
- Abdominal Dissection - trauma (or vascular if immediately available)
BOA
Mother & Baby workflow File:BOA Mother-Baby Workflow 7 14 20 (1).pdf
Brain Death
- Admit to the service who would have cared for the primary illness or injury
- Trauma - trauma patient
- Neurology - intracranial hemorrhage, stroke
- IM/FM - medical/cardiac cause
- Peds/PICU - all peds
- Admitting service should notify organ donation agency
Breast abscess/mastitis
- Breast Abscess Pathway
- Abscess
- ED aspirating (POCUS if needed)
- If you need a formal US after hours to confirm abscess, order "US Chest (R or L)" STAT [radiology only reads "Chest US", BDC only reads "Breast US"]
- Needle aspiration, send wound culture
- Standard care is needle aspiration 2x prior to I&D
- Discharge with PO antibiotics
- Keflex, dicloxacillin if lactating, bactrim or doxycycline if concern for MRSA
- Follow-up:
- DHS: ED Request for Specialty Appointment: Surgery-Breast for the following Tuesday (in 7-14 days)
- OOP: PCP in 7 days
- ED aspirating (POCUS if needed)
- If sending to BDC for needle aspiration
- 7a-3:30p (DHS or OOP) call BDC at x68178 to add case (fellow p3386, alt# x67406)
- Place ORDER for: "US Breast (R or L) STAT" and "US Drainage Abscess or Cyst" and note location of suspected abscess (X o'clock, X cm from nipple)
- Patient will return to the ED from BDC post-procedure
- BDC will arrange f/up with Breast Surgery Clinic if DHS, patient to f/up with PCP if OOP
- Start PO Antibiotics
- Keflex, dicloxacillin if lactating, bactrim or doxycycline if concern for MRSA
- Afterhours DHS Patients:
- Place FUTURE ORDER for: "US Breast (R or L) URGENT" and "US Drainage Abscess or Cyst" and note location of suspected abscess (X o'clock, X cm from nipple)
- Message Har-BDC message pool for appt
- BDC will arrange f/up with Breast Surgery Clinic if DHS, PCP if OOP
- Start PO Antibiotics
- Keflex, dicloxacillin if lactating, bactrim or doxycycline if concern for MRSA
- BDC will schedule follow-up for DHS patients or instruct OOP patients to f/up with PCP
- Afterhours OOP Patients: can consult surgery for the I&D; will need to f/up with PCP for outpatient drainage
- 7a-3:30p (DHS or OOP) call BDC at x68178 to add case (fellow p3386, alt# x67406)
- Needs I&D (failed needle aspiration(s) or overlying skin is unhealthy)
- I&D can be done by either ED or Breast Surgery (consult Trauma afterhours)
- Follow-up:
- DHS: ED Request for Specialty Appointment: Surgery-Breast for the following Tuesday (in 7-14 days)
- OOP: PCP in 7 days
- Septic Patient
- Initiate IV antibiotics
- For mastitis/cellulitis requiring IV antibiotics, admit to IM/FM
- For patients needing operative intervention, admit to Breast Surgery (covered by trauma from 7p to 7a)
- Abscess
- Schedule into BDC if:
- Palpable mass persists after 14-21 days, ultrasound and needle biopsy should be performed of solid components by radiology department
- Recurrent mastitis/abscess, or chronic granulomatous mastitis
- DHS expected practice and agreed upon by Radiology, Acute Care Surgery, Breast Surgery, EM: 2021 DHS Best Practice - Mastitis-Breast Abscess
Breast mass/malignancy
- DHS Empaneled/DHS Eligible Breast mass concerning for malignancy (THIS PATHWAY IS THE FASTEST WAY TO EXPEDITE A WORKUP)
- OOP - direct patient to their in-plan PCP for coordination of care
- OPTION 1 - NO BIOPSY-PROVEN DIAGNOSIS - Breast Diagnostic Center for imaging
- OPTION 1a - Suspicious for malignancy with NO obvious METASTASES
- Order Bilateral Mammogram and Unilateral US - future visit within 2 weeks
- "MG Mammogram Diagnostic" order set: "Mammogram Digital Diagnostic Bilateral URGENT" and "US Breast (R or L) URGENT"; Order detail must include chief complaint, relevant med/fam hx, location of mass (X o'clock, X cm from nipple)
- Message Har-BDC message pool and PCP (send to Reg 6 if no PCP)
- BDC will perform imaging, biopsy, and arrange f/up with Breast Surgery Clinic
- Order Bilateral Mammogram and Unilateral US - future visit within 2 weeks
- OPTON 1b - Suspicious for malignancy WITH obvious METASTASES (excludes local axillary lymph node spread)
- Order Bilateral Mammogram and Unilateral US - future visit within 1 week
- "Mammogram Digital Diagnostic Bilateral URGENT" and "US Breast (R or L) URGENT"; Order detail must include chief complaint, relevant med/fam hx, location of mass (X o'clock, X cm from nipple)
- Message Har-BDC message pool, PCP (send to Reg 6 if no PCP)
- Page oncology to expedite outpatient workup
- ED Request for Specialty Appointment: Oncology-New in the timeframe recommend by Oncology consultant
- BDC will perform the imaging, biopsy, and the patient will f/up with Oncology Clinic (NOT Breast Surgery)
- Order Bilateral Mammogram and Unilateral US - future visit within 1 week
- OPTION 2 - Newly diagnosed breast cancer WITH A BIOPSY-PROVEN DIAGNOSIS
- OPTION 2a - BIOPSY CONFIRMED WITHOUT obvious METASTATIC disease (excluding local axillary lymph node spread
- Pt MUST obtain records (CD images, path slides, reports)
- If the patient does not have BOTH imaging and path results, they must go to Breast Diagnostic Center first
- ED Request for Specialty Appointment: Surgery-Breast Oncology in 7-14 days
- Pt MUST obtain records (CD images, path slides, reports)
- OPTION 2b - BIOPSY CONFIRMED WITH obvious METASTATIC disease
- Page oncology to expedite outpatient workup
- ED Request for Specialty Appointment: Oncology-New in the timeframe recommend by Oncology consultant
- BDC will perform the imaging, biopsy, and the patient will f/up with Oncology Clinic (NOT Breast Surgery)
- Page oncology to expedite outpatient workup
- Random Scenarios
- If unsure if a mass or abscess, schedule into BDC and order the imaging
- Mastalgia, breast lesion needing excision for non-malignant lesion, need for cancer surveillance after losing insurance elsewhere - NERF/message PCP for e-consult
Burns
- Transfer to burn center AFTER Trauma service consultation if meets ABA burn center referral criteria
- Partial thickness burns greater than 10% total body surface area (TBSA)
- Burns that involve the face, hands, feet, genitalia, perineum, or major joints
- Third degree burns in any age group
- Electrical burns, including lightning injury
- Chemical burns
- Inhalation injury
- Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality
- Any patient with burns and concomitant trauma (such as fractures) in which the burn injury poses the greatest risk of morbidity or mortality. In such cases, if the trauma poses the greater immediate risk, the patient may be initially stabilized in a trauma center before being transferred to a burn unit. Physician judgment will be necessary in such situations and should be in concert with the regional medical control plan and triage protocols
- Burned children in hospitals without qualified personnel or equipment for the care of children
- Burn injury in patients who will require special social, emotional, or rehabilitative intervention.
- LAG cannot refuse transfers
Cardiology
REVIEW
- Cardiology consults and admissions:
- For quick questions during business hours, CORE fellow p1035 (follow up, CORE vs Cteam admission, etc.)
- For Admits, contact Third call p6534
- For anything else (potential STEMI, not sure what a patient has, not sure what the rhythm is, discharge coordination when CORE isn’t here, etc.) --> Fellow consult pager - p6493
- Any issues reaching on-call fellow, 1) check MedHub and call the on-call fellow, or 2) call the CCU, or 3) consider contacting attending
- Starting 10/4: CORE NP taking CORE admits until 8p Mon - Thurs
CHF
- If estimated <2 midnight stay, place in Cardiology Observation Rapid Evaluation area (CORE) CORE
- Admit any patients with anasarca (including abdominal or scrotal edema)
- If estimated >2 midnight stay:
- Admit to IM/FM (tele/PCU) if all of the following are met:
- Low suspicion for ACS (as determined by ED attending)
- HR < 110
- BP > 110
- Creatinine <2.0 (unless ESRD on HD)
- No BiPAP required at any time in the ED
- Admit to Cardiology (C-team) if the above criteria are not met or the patient needs ICU care
- Admit to IM/FM (tele/PCU) if all of the following are met:
Cellulitis, Abscess, NSTI
- Cellulitis
- IM/FM
- EXCEPTION: Hand Call (plastic surgery or ortho) - upper extremity cellulitis (hand to AC, or proximal to AC if primarily below) or deep space hand
- Soft tissue abscess
- Trauma - all except face, neck, mouth, or distal arms; even if drained in the ED
- Spine call - epidural abscess
- NSTI - trauma surgery
- Maxillofacial cellulitis or abscess
- Optho - periorbital/orbital
- OMFS - odontogenic infection or facial cellulitis secondary to dental
- "Tooth Call" pager: 800-233-7231 x32831 (per ENT 10-2-16)
- ENT - dental infection with facial cellulitis AND neck extension WITH risk of rapid loss of airway, deep space neck infection, or sinus infection
- Face call - all other maxillofacial infections
Dialysis fistula/graft problem (e.g. bleeding or thrombosed)
- Trauma (or vascular if immediately available) if needs immediate operative intervention (uncontrolled bleeding)
- Require IR
- If unable to perform outpatient, admit to IM/FM
- IM/FM (with vascular and nephrology) if requires more than IR
- Less than 30 days post-op - trauma consult in the ED
Decubitus Ulcers
- Trauma/ACS - admit when patients require hospitalization primarily for surgical debridement of decubitus ulcers
- IM/FM - admit when patients require hospitalization primarily for management of medical problems but also have decubitus ulcers
- 11/1/2022 - Drs. Thomas, Putnam, Schickedanz, Goolsby
Deep venous thrombosis
- DVT
- Vascular Surgery (through Trauma Surgery afterhours) for phlegmasia or subsequent compartment syndrome
- Phlegmasia alba dolens painful swollen white leg from early arterial compromise
- Phlegmasia cerulea dolens = painful swollen cyanotic leg, bullae and necrosis from later arterial compromise
- Heparin 80-100U/kg followed by infusion of 15-18U/kg/hr
- Consider IR for thrombectomy:
- Acute symptom onset of 14 days or less in the target limb.
- Presence of proximal DVT (inferior vena cava, iliac vein, common femoral vein, deep femoral vein, and femoral vein) that was objectively diagnosed with CT and/or US scan
- Symptomatic DVT (pain, neurological deficit) or impairment of the tissue perfusion (phlegmasia) and less than 14 days' duration
- Symptomatic DVT defined as meeting at least one of the following clinical indicators:
- rVCSS Pain Score ≥2
- New edema of calf or thigh (CEAP ≥3)
- Limited mobility or bed bound due to pain / swelling
- Symptomatic DVT defined as meeting at least one of the following clinical indicators:
- Acute symptom onset of 14 days or less in the target limb.
- If needs admission, IM/FM
- <30-day post-op, admit to surgical service who performed the operation
- OB/Gyn - pregnant, <6-weeks post-partum, due to gyn malignancy
- Vascular Surgery (through Trauma Surgery afterhours) for phlegmasia or subsequent compartment syndrome
Delirium/Dementia
- Acute delirium
- IM/FM
- Dementia
- Dr. Kronfeld, Director of Inpt Neuro, 7/2022
- Typically, concern for gradual onset dementia does not warrant admission solely for workup
- Discharge with neuro clinic follow-up if neurology recommends outpatient evaluation of the patient
- May need to consider Placement Pathway (consult SW, PT/OT, UR, and involve ED AOD ASAP)
- If rapidly progressive dementia, consider UDS, psych consult, LP, and inpatient admission/MRI
- Typically, concern for gradual onset dementia does not warrant admission solely for workup
- If admission is warranted:
- Neuro - new onset or previously undiagnosed
- IM/FM - new onset with one or more complicating medical condition
- Dr. Kronfeld, Director of Inpt Neuro, 7/2022
Diabetic Foot Infections
- Effective 10-4-2023: all diabetic foot infections will go to IM/FM with limb salvage consultation (Dr. Thomas, IM Chair; Dr. Miller, Limb Salvage)
- Hold antibiotics until surgery evaluation unless the patient is septic or has rapidly progressing infection
- Consult Limb Salvage (or Trauma/ACS after-hours) if being admitted for another primary medical condition but also has a diabetic foot infection (Confirmed with Dr. Putnam 7-15-2021)
Disposition Problems
- Patients with placement needs, see Harbor:Placement_patients for more detailed tips
- Consult SW early, many resources only available during business hours
- Offer family option of Harbor:Home_Health for PT/OT, home safety evals if can wait couple business days
- If unable to safely discharge, then need to admit (DHS) or transfer (if OOP) for placement, via Interqual request
- Admit to IM/FM for DHS patients that need long-term placement unless otherwise directed by UR
- If unable to transfer to patient's OOP network or unable to authorization to admit to IM/FM then:
- Ensure UR Director is aware via UR nurse.
- Let Harbor:DEM_Admin_on_Duty_(AOD) know, as may need higher level discussion
- EXCEPTIONS:
- Patient develops a complication from a medical or surgical problem and is already followed by that particular service in the outpatient setting should be admitted to that service
- Problem is solely surgical without complicating medical condition, admit to that surgical service (eg, cannot care for self due to fracture, admit to ortho)
GI Bleeding
- IM/FM: all patients with GI bleeding who require admission, including post-endoscopy
- GI should evaluate immediately if patient hemodynamically unstable or requiring massive transfusion; admit to MICU with Trauma / ACS consultation.
- Admit to Surgery only if established surgical patient that has GI bleeding potentially related to a surgical procedure
(Chair IM, Chief Trauma 5-8-20)
Gyn
- DRAFT
- D&C's
- Indications for vacuum aspiration: r/o ectopic, incomplete miscarriage (no FHTs), active miscarriage
- Gyn Clinic:
- Patients who can be reasonably managed on an outpt basis should have D&C in gyn clinic
- Patients requesting termination of pregnancy can be seen at ROC clinic on Wednesdays
- ED D&C indications:
- Patients experiencing symptoms that would generally necessitate taking to the OR solely for a D&C but are stable
- Patients who have extenuating barriers to clinic follow-up
- OB can perform paracervical block in the ED (no procedural sedation)
- Patients generally need to be monitored for 30 min post D&C
- Gyn to provide pictorial for appropriate amount of post-procedural bleeding and will re-eval pt if there is concern from the ED provider or RN
- NB/JL - need written policy ... same population as clinic; do in clinic during clinic hours; standard work in clinic; no sedation
- OR:
- Any patient with massive hemorrhage, hemodynamic instability, or expected prolonged recovery period
- Gyn Clinic:
- Indications for vacuum aspiration: r/o ectopic, incomplete miscarriage (no FHTs), active miscarriage
- D&C's
Hand Injuries & Infections
- Fractures of hand and forearm: Ortho
- EXCEPTION - isolated distal phalanx fractures: Hand call (plastics & ortho)
- Trauma patient need clearance by Trauma Surgery prior to admission
- Soft tissue injuries or infection up to elbow WITHOUT fracture: Hand call (plastics & ortho)
- Replant injuries will always be ORTHO as a fracture is involved
Hip Fractures
Click here for ED Pathway: Harbor Hip Fracture Pathway
- Suggested pre-op workup (UCSF Guideline):
- XR hip, pelvis, femur
- CBC, Chem 10, INR, Vitamin D, T&S
- CXR & EKG if history of heart or lung problems
Hypertension
- Patients with hypertension as a COMPLICATING MEDICAL CONDITION will be admitted to Internal Medicine/Family Medicine only if the hypertension is the primary reason for admission; otherwise, Nephrology may be consulted to assist with management.
Intracranial mass lesions
- Non-hemorrhagic intracranial masses
- Neuro with NS consult: new solitary lesion without hemorrhage
- IM/FM with NS consult: non-hemorrhagic mass WITH complicating medical condition OR likely metastatic disease
- Patients with known mass will be admitted to the service that manages them on outpt basis (eg, IM with oncology for glioma, Neuro for MS)
- Neurosurgery: hemorrhagic OR non-hemorrhagic mass that require emergent surgical intervention or ICP monitor will be admitted to Neurosurgery, regardless of the presence of a Complicating Medical Condition.
- ED will call NS with the specific question, "Is it surgical or does it need an ICP monitor?” If no, then admit to neuro (ED does not need to wait for the full consult, just the answer to the pointed question).
- Trauma: Trauma surgery has right of refusal for admitting any patients with a traumatic mechanism.
- 6/2023: Drs. Dhall (NS), Kronfeld (Neuro), Putnam (Trauma), & Chappell (ED)
Lower back pain
- Admit IM/FM pain control with no neuro deficits
- Could consider NS consult
- Neurosurgery: LBP with acute weakness, bowel/bladder incontinence, or requiring surgical intervention
Malignant Hyperthermia
- Call OR front desk x65200 to get the Malignant Hyperthermia Cart
Maxillofacial trauma
- Trauma: any maxillofacial traumatic injuries requiring admission
- Face Call: isolated non-traumatic maxillofacial diagnoses requiring surgical intervention
- Optho: isolated glob injury (eg, globe rupture)
Meningitis
- IM/FM
- Neuro can be consulted for diagnostic and management assistance
Neurosurgery
- Consult NS on any patient presenting within 30 days of surgery regardless of reason for visit (Dr. Dhall, NS Chair, 4/1/22)
NSTEMI
- C-team: if appears to be secondary to ACS or CHF
- IM/FM: if appears to be secondary to non-cardiovascular cause (eg, sepsis)
- Trauma: if appears to be secondary to a traumatic injury (eg, cardiac contusion after a motor vehicle accident) and NOT the etiology of the trauma (eg, cardiac syncope leading to a motor vehicle accident)
- Determination of the most likely cause of the NSTEMI will be made by the ED Attending
Optic Neuritis
- Admit to Neurology if requiring inpatient admission and alternate ophthalmologic condition is not suspected
Dr. Kronfeld (Director Inpatient Neuro) 2/9/2022
Osteomyelitis requiring admission
- Hand Call: hand and forearm
- Ortho: all other extremity osteo, especially if underlying hardware
- NS: osteo of the spine WITH acute weakness, numbness, or bowel/bladder incontinence
- IM/FM: all other osteo locations (including spine without neuro deficit)
Painless Jaundice
- Consider Expedited Work-up Clinic if stable for outpatient evaluation
- Message PCP if DHS empaneled
- CCC for EWC if the patient does not have a PCP
- IM/FM if requiring admission
Pancreatitis
- Trauma/ACS: if gallstones present on ultrasound
- Bedside US requires: gallbaldder wall thickness, comment on pericholecystic fluid, comment on gallstones, and diameter of the common bile duct or common hepatic duct
- If all 4 items are not present, formal US should be obtained
- Pancreatitis without gallstones, admit to IM/FM
Pathologic Fractures
- HUCLA can take care of small benign bone tumors (like UBC's or ABC's) with fracture, fracture through a known primary, or fracture through a met of known primary.
- We don't have orthopaedic oncology at Harbor.
- Transfer to USC if unclear whether new primary (not a met) because the fixation method and approach changes based on the primary
- If unclear, escalate to the HUMC Ortho Attending 24/7
Dr. Badkoobehi 12/14/2022
PEDIATRICS

Placement Patients
Pregnant Patients
- Consult OB for all pregnant patient requiring admission
- OB will admit all pregnant patients unless the patient has a medical or surgical condition that requires or is likely to require active management beyond the scope of practice of the Obstetrics and Gynecology service
- If the ED and OB attendings disagree with the admission service, the final decision is made by the OB attending
Pulmonary Embolus
- For all Confirmed PE or DVT with findings suggestive of PE (Clot in transit or right heart thrombi on TTE/TEE) but unable to obtain CTPA, risk stratify patient for PE Response Team Activation using ED PERT Activation Algorithm 2026.
- Risk Stratification
- Harbor UCLA's PERT Program currently uses the European Society of Cardiology (ESC) 2019 Guidelines for risk stratification to help determine treatment options and level of care:
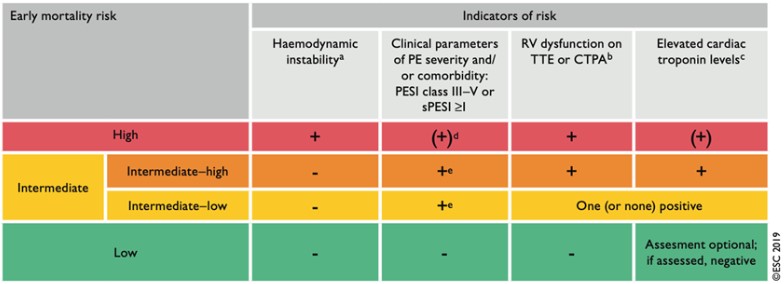
- Definition of hemodynamic instability for risk stratification
- Cardiac arrest and need for cardiopulmonary resuscitation.
- Obstructive shock defined as a systolic blood pressure (BP) < 90 mmHg or vasopressors required to achieve a bp > 90 mmHg despite adequate filling status and end-organ hypoperfusion (altered mental status; cold clammy skin; oliguria/anuria; increased serum lactate)
- Persistent hypotension with a systolic BP < 90 mmHg or systolic BP drop > 40 mmHg, lasting longer than 15 minutes and not caused by new-onset arrhythmia, hypovolemia, or sepsis
- sPESI
- Harbor UCLA's PERT Program currently uses the European Society of Cardiology (ESC) 2019 Guidelines for risk stratification to help determine treatment options and level of care:
- While you’re waiting for PERT you can…
- Begin anticoagulation if no absolute contraindication (see reference below)
- Strongly consider obtaining a head CT for patients who have underlying malignancy prior to starting anticoagulation
- Ensure the following labs are drawn and studies are ordered
- CBC w/diff, CMP, PTT/INR/Anti-Xa, troponin, BNP, lactate
- Bilateral lower extremity ultrasounds (consider upper extremity if patient has a chronic central line in place or symptomatic arms)
- TTE with PERT protocol
- Ensure at least x2 large bore PIVs; if central line is required for pressors then avoid non-compressible sites (e.g. subclavian vein)
- Assess for thrombolysis contraindications (see table below)
- Anticoagulation Guidelines
- Unfractionated Heparin (UFH)
- Utilize Heparin Drip DVT/PE per Pharmacy subphase order set
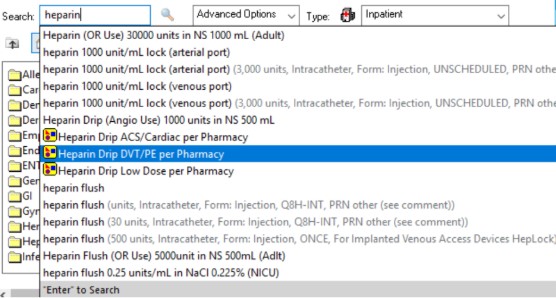
- Note, this order set automatically includes a bolus of heparin. If this is not desired such as in patients who are at increased risk of bleeding, please unclick the checked off box
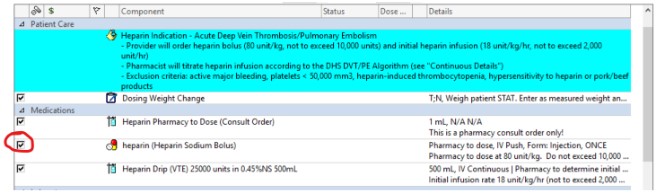
- Utilize Heparin Drip DVT/PE per Pharmacy subphase order set
- Low Molecular Weight Heparin (LMWH): Enoxaparin 1 mg/kg q12h (avoid if CrCl < 30mL/min)
- DOACs (Low Risk Only):
- Rivaroxaban: 15 mg PO BID x 21 days -> 20 mg daily (avoid if CrCl < 30mL/min)
- Apixaban: 10 mg PO BID x 7 days -> 5 mg BID
- Note when able, Apixaban is favored over Rivaroxaban given decreased bleeding risk
- Unfractionated Heparin (UFH)
- Thrombolytic Contraindications




- Frequently Asked Questions
- PERT is not responding. What should I do?
- PERT should respond within 15 minutes. Repage x 1 and escalate to Pulmonary Consultation attending on call if no response (see MedHub for attending name and contact number).
- I consulted PERT. Do I need to reach out to IR, Cardiology, or Surgery for my patient to be considered for catheter-based or surgical intervention?
- No; PERT will coordinate and consult all the other members of the PERT program as needed on a case-by-case basis.
- I have a high-risk PE patient who is unstable and/or in extremis. Do I need to wait for PERT prior to giving thrombolytics?
- If the patient can be stabilized with vasopressors, holding off on the administration of thrombolytics until PERT is able to able to provide input to the patient’s care is preferred.
- If you feel you cannot wait for this response, then perform a quick assessment for contraindications for thrombolytic administration prior to starting the administration.
- My patient has a DVT. Do I activate PERT?
- No. If you later find a PE in your workup, then please follow the algorithm and determine if PERT consult is appropriate.
- For symptomatic DVTs, both IR and Vascular Surgery can help with the assessment and additional management strategies.
- I am unable to get a CTPA but am worried about a PE. Do I activate PERT?
- No. The PERT program is intended to assist in the care of patients with a confirmed PE in the intermediate- or high-risk range that might benefit from more advanced therapy beyond anticoagulation alone.
- If you need assistance with assessing the patient and would like additional help, please contact the Pulmonary Consultation service (pager 310-501-5194).
- A patient with a prior PE returns to the ED. Should I activate PERT?
- The answer is it depends...
- If they are coming in with a new PE event and have features consistent with an intermediate- or high-risk features, activate PERT.
- If they are coming in with a concern for anticoagulant failure in the setting of the original PE management, bleeding, or other concerns, PERT should not be activated. Consultation of medical subspecialty service including Hematology or Pulmonary can be obtained depending on the concern.
- The answer is it depends...
- I have a question about anticoagulation, but the patient does not have an acute PE. Who do I consult?
- Hematology/Oncology would be the consultation team to start with if there are questions specifically directed at anticoagulation choices alone.
- PERT is not responding. What should I do?
Drs. Vintch/Chappell/Grohmann 2-2026
Pyelonephritis
- Men and non-pregnant women, admit to IM/FM
- Urology: pyelonephritis associated with nephrolithiasis, urinary stents, obstructive uropathy, or nephrostomies
- If they have a Complicating Medical Condition, they will be admitted to Internal Medicine/Family Medicine with consultation by Urology
- OB/Gyn: pregnant women with pyelonephritis
- If they have a Complicating Medical Condition, they will be admitted to Internal Medicine/Family Medicine with consultation by OB/Gyn
Re-implant (Replant)
ROSC
- C-team: presumed cardiac etiology of cardiac arrest
- MICU: presumed non-cardiac etiology of cardiac arrest
- The presumed etiology will be determined by the ED Attending physician. Initiate TTM, consider CT head, with post ROSC care
Septic Arthritis
- Orthopedics unless the patient has systemic sepsis or complicating medical conditions
- IM/FM with ortho consult if CMC or sepsis
Spinal Injuries
- Trauma/ACS: All cervical, thoracic, or lumbar injuries
Stroke
- Neurology: All strokes (ischemic or hemorrhagic) EXCEPT:
- Trauma/ACS: traumatic ICH (if cleared by Trauma Surgery, admit to Neurosurgery)
- Non-traumatic ICH:
- Simultaneously consult NEURO and NEUROSURGERY
- Admit to Neurosurgery if the require emergent operative neurosurgical intervention or ICP monitor
- ED will call NS with the specific question, "Is it surgical or does it need an ICP monitor?” If no, then admit to neuro (ED does not need to wait for the full consult, just the answer to the pointed question).
- Neurology admit with NS consult: non-aneurysmal SAH or non-massive ICH (including post-tPA hemorrhage)
- Admit to Neurosurgery if the require emergent operative neurosurgical intervention or ICP monitor
- Simultaneously consult NEURO and NEUROSURGERY
- IM/FM with neurology if complicating medical condition
- 6/2023: Drs. Dhall (NS), Kronfeld (Neuro), Putnam (Trauma), & Chappell (ED)
Surgical Specialty Consults
- ALL surgical admissions (acute care or trauma) go to the "Surgery - Trauma" service
- For surgical subspecialty consults:
- Page Trauma/ACS
- During daytime hours, you can directly page the specialty service if you need a more rapid decision, especially if already known to specialty service
Thyroid Masses
- Refer to endocrinology
Trauma patients
- Trauma/ACS: will admit all multi-system trauma including fractures and must clear any TTA1 or TTA2 patients prior to admission to other services
- Hip Fractures: see Hip Fractures guideline
- Ortho: isolated traumatic fractures once cleared by trauma
Vaginal Bleeding
- Gyn: symptomatic anemia from vaginal bleeding requiring extended stay OR greater than 2U pRBC transfusion
See Also
References
Mandatory Reporting of Adverse Events
There are events which we must report to the state in a timely fashion or face being penalized by State Licensing. Below are some general guidelines for what to report. Please make sure that the ED attending is aware of these events and documents their involvement in the record.
Events must be reported within 4 hours to both of the following:
- PSN (Patient Safety Net)
- Risk Management x2168
Events to be Reported
- Procedure performed on a wrong body part, patient, or the wrong procedure all together.
- Retention of a foreign object (e.g. central line guidewire)
- Patient death or serious disability through any actions or errors which are not an expected part of the patients medical condition or treatment, including elopement of an incompetent individual or minor, or an assault.
- Visitor or staff death or severe disability while on hospital grounds for any reason.
- An infant discharged to the wrong person.
- A maternal death or serious disability within 42 days post delivery
- Any instance of care ordered by or provided by someone impersonating a physician, nurse, pharmacist, or other licensed health care provider.
- Any abduction or sexual assault of anyone on hospital grounds.
(Ref: Reporting Form – Adverse Events -Julie Rees)
(Hospital policies 612A, 612B 5/14)
Safe Pain Management Program
We will be shortly launching the implementation of the Safe Pain Medication Prescribing Guidelines, a Los Angeles county-wide project to decrease inappropriate opioid prescriptions from the ED and other settings. Patients will receive upon discharge a color pamphlet (English or Spanish) explaining the project, including messages about how stolen prescriptions need to be reported to the police, that the ED does not refill pain pills and that pain pills for chronic pain should really come from a single, continuity provider. Residents, NPs, and nursing staff got some in-depth lectures about this. (Dir Adult ED 10/14/14)
Boarding
Boarding Patients Sent from Clinic
Just a reminder to the seniors in the Emergency Department running the board: the correct procedure for patients admitted from clinic who do not need a monitored bed, especially when the clinic is closing, is for the clinic to contact the patient flow facilitator to assist in locating a bed in the hospital, and only contact the emergency department to board the patient if the flow facilitator cannot make other arrangements.
Monitored bed patients can be sent from the clinic to the emergency department to board when we are out of monitored beds. If it doesn't sound like the patient needs a monitored bed, please talk to the ED attending.
Triaging Clinic Patients
Because we have a large volume of patients waiting at any given time, many of whom are quite ill, we support independent medical decision-making about whether a patient coming from a clinic needs immediate attention or can safely wait to be triaged.
We do ask however that when triaging clinic patients, you follow the same protocol we use for ambulance patients (see below 1.9.2). Specifically, should a resident decide that a clinic patient is stable to go wait in the waiting room, they discuss it with the attending and document that decision in the medical record. You can use the same autotext you'd use for an ambulance patient.
Regarding sending the patient to RME: we have no workflow that allows a patient to be placed directly into RME - please don't ask the nursing staff to do this. If you decide that the patient is not stable to go to the waiting room and be triaged, then please keep them in the AAED.
(Dir. OPS, February 03, 2015)
Template:Triaging Ambulance Patients
Family Viewing of Deceased Patients
If you have a death in the ED, please don't direct family to the morgue and don't promise body viewing. If the death is potentially a coroner's case, with an unclear cause of death or concerns for possible criminal activity (violence, hit and run, etc.), the family may not be allowed near the body for concerns of evidentiary integrity. For any death that we will be disclosing to the family, the ED social worker should be present to handle the details of discussing body and funeral preparations with the family.
Family Bereavement Resources
How to access the bereavement packet if needed.
- Go to home page for Harbor/UCLA and click on Departments/Site pages
- Once the page comes up, look in the second column for Patient Education
- Click on Patient Education
- Once the page comes up, look for Patient Handouts
- Click on Patient Handouts
- Once page comes up, scroll down to Bereavement packet; it is available in English, Spanish, and Korean.
Law Enforcement Escorting Patients Out Of the Emergency Department
Because of the potential conflicts with EMTALA law, it is important that a physician be involved in any decision to remove any patient or potential patient from the emergency department. For this reason, any time law enforcement is either requested by nursing staff, or decides on its own, to escort a patient from the emergency department (including the waiting room), an attending physician should be notified and agree with (and document) the decision. The House Supervisor should also be notified (x3434) before involving law enforcement. Documentation should specifically state that the patient has had a medical screening exam and does not have an emergency medical condition, or if there is an emergency medical condition that it has been appropriately stabilized. Obviously, it should also be safe for the patient to be removed from the emergency department.
Dir AED 5/26/16
Orders on Admitted Patients
Recently we had problems in the care of a patient due to both the emergency physician and the admitting team writing non-emergent orders on the patient at the same time.
Please do not write orders an admitted patient unless it is an emergency. If you do write an order on the an admitted patient, please communicate this as soon as reasonably possible to the admitting team. If nursing staff request that you write non-emergent orders on an admitted patient, please direct them to call the admitting team.
Admission officially occurs at the time you place the order "Request for Admit", and only after you've communicated with the admitting team about admission (or made a reasonable attempt to do so)
Dir OPS 5/5/15
On Call Plan - Emergency Department Attending Physicians
When it becomes clear for any reason that an Attending Physician in the Adult or Pediatric ED will be unable to cover a scheduled shift due to illness or personal emergency, that physician should:
- Send out a group wide email in an attempt to find coverage, as time permits.
- Outside business hours, contact the attending on duty in emergency department, who will notify involved physicians that the shift extension backup plan is in effect (see section 5 below). Contact information for all ED physicians is available on our intranet website http://www.emedharbor.edu/private/
- During business hours, call the Department Offices at 310 222-3500 and inform Maria Figueroa, or if unavailable, Juno Chen. Maria (or Juno) will contact the Chair, or in his absence, one of the Vice Chairs, who will initiate an e-mail attempt to arrange coverage. If no coverage is found, the Chair or Vice Chairs will notify the attending in the emergency department to activate the shift extension backup plan.
- Part time hourly physicians and volunteer physicians are not obligated under this plan, but will be compensated for their time per their usual agreement should they decide to cover additional hours under this plan.
- Shift Extension Back-up Plan: When no coverage can be found - the physicians working the shifts before and after the missed shift will extend their shifts to 12 hours to cover the missed shift. AAED A-team physicians are responsible to cover A-team absences and AAED B-Team for B-Team absences, and PED team physicians cover PEDS team absences.
- In the event one of the covering physicians is a part-time physician and unable to extend their shift, the physician from the opposite team should extend their shift to 12 hours to help cover the missed shift.
- A full-time faculty member or Fellow will generally be responsible for making up the first 2 shifts missed from any single incident. At the discretion of the Chair, the requirement to make up subsequent shifts may be waived.
- Faculty will not be required to pay back specific individuals who worked their missed shifts. Shift pay back will be accomplished through the regular scheduling process.
- Faculty working extra to cover missed shifts should notify the scheduler to ensure appropriate credit is given.
(Dir of OPS 6/2/15)
Trauma Activations
In addition to the standard trauma activation criteria published on a badge card that everyone should carry and refer to, the Trauma Service can be activated in patients not meeting trauma criteria to help in several ways:
- Getting CT scans READ quickly (Trauma will read them)
- Getting lots of extra hands to do whatever needs to be done for the patient.
- Getting surgical decisions made more quickly.
You can even activate the trauma service if you have a non-trauma patient that needs emergent surgical intervention.
All of these decisions are covered under "ED Judgment"
(Dir OPS 7/15)
RME/TRIAGE
Criteria for an immediate transfer to Chest Pain Room
- Router RN identifies patient with Triage Priority CP
- Router RN calls CP Triage RN.
- CP Triage RN performs assessment to determine if patient meets criteria for ECG:
- Chest, arm, neck, jaw, upper back, or epigastric, pain/pressure/heaviness/discomfort concerning for a cardiac etiology, in a patient > 30 yrs old.
- Shortness of breath, weakness, or arm/hand numbness, in a patient > 30 yrs old, concerning for a cardiac etiology and without another explanation
- Nausea, lightheadedness, “indigestion”, or "dizziness" in any diabetic OR elderly patient (>65 yrs) concerning for a cardiac etiology and without another explanation
- Syncope with age > 30 yrs
- If clinical concern persists despite absence of 1-4
TRANSFER TO CHEST PAIN ROOM, PERFORM IMMEDIATE ECG, AND THEN NOTIFY NP, x23219.
NP Consultation with the Attending Physician
Nurse Practitioners working in the RME or Emergency Department should seek consultation with an Attending Physician as is outlined in the Physician Consultation Guidelines.
All admissions performed by an NP require an Attending Admission Note (see "Admit Process" for contents of note).
If an NP wishes to disposition any patient they have consulted an attending physician on (even if the patient's condition is on the independent disposition list), the attending MUST sign the chart. NPs will refer all such charts to he attending for signature. It is expected that on any case that an attending has been consulted, the NP will discuss the disposition of the patient with the attending before actual disposition.
It is at the discretion of the attending whether or not to personally evaluate the patient, however the attending physician will be responsible for the care delivered to the patient. Patients who are under the care of an NP but have been discussed with an attending physician may have the attending's name placed in the attending column but should NOT be given a team color. The NP should leave their name on the patient on the track.
(Dir OPS 7/15)
Designation of Patients in Rapid Medical Screening Exam (RME) Area
Nurse Practitioners (NPs) in RME, the RME Charge Nurse, or the ED Attending can designate patients in RME as belonging to an AAED team. In order to do this, the patient should be assigned a team color on the usual rotating basis, have the NP's name removed from the resident/attending/or intern columns, and place the patient in a designated AAED bed.
Once a patient has been placed on an AAED team, NPs should not write any more orders for that patient. Any further orders will be written by the AAED team.
Patients who are under the care of an NP but have been discussed with an attending physician may have the attending's name placed in the attending column but should NOT be given a team color. The NP should leave their name on the patient. The nurse practitioner should forward the documentation for attending signature.
(ALL MDS/NPS/NURSING DIRECTOR ED 7/14)
EKG Screening by NPs
- CP patient from Triage needs an ECG in RME 11 CP room.
- ECG tech hands ECG to NP.
- NP does the electronic ECG screen in ORCHID for ECGs that say “Normal Sinus Rhythm.”
- For ECGs that say anything else, if the ECG is already uploaded into ORCHID, the NP screening chest pain patients can just call the ED attending (x23202 or 23206) for the electronic ECG screen. Otherwise if the ECG is not yet uploaded, the NP will have to walk over the ECG to an ED attending. If there is an RME physician, then that physician can perform the electronic ECG screen.
Bed Huddles – RME
Every morning at 7:30 am and every evening at 7:30 pm A bed huddle between the RME nurse practitioners and RME nursing staff should occur.. The charge nurse should initiate by gathering nursing staff and NPs into the NP room. The following should be done during the huddle:
- Identify the charge nurse for RME that day and write his/her phone on the white board
- Find out from charge if we are short staffed
- Find out who your staff is for RME beds, and room 12
- Let them know which NP is the screening /chest pain NP. If you are short that day also let them know.
- Remind them how chest pain process should run
(Lead NP 5/15)
Attending Sign Out of RME Patients
Occasionally the physician working in RME may need to sign out a patient to the AAED in attending if no RME attending a scheduled for the following shift. In the instance where the RME physician saw a patient outside the NP scope, we are asking that the RME physician sign out the plan to both the NP and the AAED attending. That way if the NP has any questions, or if any issues come up, they can have an attending to get guidance from that already knows the patient.
EMS
Responding to a Helicopter Landing
- Requires 2-3 trained individuals, does NOT require a physician, though one may elect to go.
- Only individuals with helicopter safety training should respond to a helicopter landing.
- Must wear following (available in radio room):
- Eye protection
- Gloves
- Ear plugs
- FOR SAFETY:
- Secure loose equipment, they may become a projectile.
- Face shields are not permitted.
- Stethoscopes are not to be worn around the neck.
- Items are not to be left on top of the gurney
Closing to EMS (ALS) Ambulances
The decision to close to ALS ambulances should be made as a joint decision by the AED charge nurse and the ED attending. Although looking at the NEDOCS score can be a helpful indicator of the level of congestion, it does not need to be the only factor that goes into determining the need to close to ALS ambulances. With our recent adjustment of the equation to calculate the NEDOCS score (we now have the accurate ED bed count in the equation) - you may find at times that you need to close at lower NEDOCS scores.
As always, the decision to close should be carefully considered, as it results in longer transport times for potentially critically ill patients.
FINANCE
Billing Credit for Attending Staff
Attending credit should be given based on documentation in following order:
- First to the attending who writes an addendum on the resident's the H&P
- If there is no attending addendum on the H&P, then credit goes next to first attending who writes the appropriate "Supervisory Review Note".
- If there is no attending addendum on the H&P or a separate Supervisory Review note or other separate attending note, then credit will be given to the attending who signed the H&P.
- For procedures-the attending specified in the procedure note will get credit for procedure billing, even if a different attending gets credit for the patient visit (E&M code).
(Dir OPS 11/13/14)
ORCHID (CERNER)
HARBOR ED POLICY MANUAL
3.0 Admissions and Consultations
3.4: Guidelines for Flow of patients between the Psychiatric and Adult Emergency Departments
- Ambulatory Patients: Patients presenting with abnormal behavior WITHOUT prior psych diagnoses or with acute ALOC are initially evaluated in the adult ED
- Patients with a known psych history and behavior consistent with their previous diagnosis, without apparent acute medical condition requiring intervention, are initially evaluated by the Psych ED
- Patients arriving by ambulance with psych complaints but not under a 5150 should be triaged by a physician in the adult ED then directed to appropriate location
- Psychiatric Consultations in the ED: patients requesting voluntary evaluation by a psychiatrist are transferred to the psych ED after medical clearance for evaluation and should be transferred to the psych ED as soon as there is space available; ED physician to psych physician discussion should occur prior to transfer
- All patients on a 5150 hold
- With ETOH>200, delirium, complicated alcohol withdrawal, drug overdose, or acute medical problems should be evaluated in the adult ED
- Require psych evaluation prior to discharge or transfer to medical unit; this should be done within 30 minutes of request for consult
- Patients in the psych ED that require medical evaluation (or re-evaluation) should be transferred to the adult ED as soon as a bed is available; prior to the transfer, the psych physician should discuss the case with the ED physician; exceptions will be made on a case-by-case basis
- Patients in the Psych ED who require treatment with sedatives and are deemed to be at risk for significant oxygen desaturation should be transferred to a monitored bed in the adult ED; these patients are co-managed by the physicians from both areas
- Psychiatric patients with chronic disorders who require placement are managed in the Psych ED
Approved June 2015, Chappell 2/22/16
21.3 Respiratory Isolation Patient Protocol
- All adult patients presenting to the DEM will be screened at the time of triage by a RN for risk factors, symptoms or complaints of respiratory/tuberculosis (TB) using the RIPT criteria in the EHR; five points or greater indicates the need for immediate initiation of the RIPT procedure.
- A mask will be placed on the patient and PA/Lateral chest x-ray will be ordered by the triage nurse with a DEM Attending on duty as ordering physician.
- The patient will be escorted to the radiology waiting area, and the triage nurse will hand off communication to the Area Charge Nurse (ACN).
- On completion of the chest x-ray, the ACN will follow-up with the R-3 or Attending Physician for interpretation of the chest x-ray. The decision to release the patient back to the waiting area or continue isolation in a designated isolation room will be made by the provider at that time.
Approved June 2015, Chappell 2/22/16
21.4 Care of Potential Myocardial Ischemia Patient in Triage
- All adult patients presenting to the DEM triage area with a chief complaint suggestive of myocardial ischemia will be screened rapidly by the Router RN to determine the need for immediate intervention using the following criteria:
- Age >35 AND chest, arm, neck, jaw pain that is described as pressure, heaviness, or discomfort.
- Age >45 AND Shortness of Breath, weakness, or arm numbness, CONCERNING FOR A CARDIAC ETIOLOGY and without other explanation
- Age > 65 AND Nausea, lightheadedness, “indigestion”, or “dizziness" CONCERNING FOR A CARDIAC ETIOLOGY and without other explanation
- Clinical concern for myocardial ischemia exists despite absence of 1-3
- If the patient meets the above criteria the Router RN will assign a triage priority of cardiac and notify the triage RN via phone; the patient will be placed in room 11 in the RME area
- The triage nurse performs the complete focused assessment and appropriately orders the EKG under the DEM Attending on duty
- Once the ECG has been completed, the triage nurse will notify the RME provider who will review the EKG
Approved June 2015, Chappell 2/22/16
21.5 Medications in Triage: Standardized Procedure
- Administration of medications in triage (MIT) is to provide timely treatment for patients arriving to the ED in pain, with fever, with dyspepsia, or N/V. Patients in pain should be offered oral analgesia at the time of triage/assessment and reassessment.
- DEM Triage RN's have received additional training in giving medications in triage and may administer medications (Acetaminophen, Ibuprofen, Aluminum hydroxide and Magnesium hydroxide antacid [Mag-Al Plus], or Ondansetron) to patients when indicated by the specific requirements of this procedure unless contra-indicated.
- PAIN: All patients who arrive to the ED Triage area will have their level of pain assessed and documented in the EMR. The pain scales used are FLACC, Numeric, and Faces, depending upon the age of the patient. Dosages for fever and/or pain shall be as follows:
- Child < 12 years of age – Acetaminophen 15mg/kg PO x 1 (max 650 mg)
- Child ≥ 12 years of age – Acetaminophen 15mg/kg PO x 1 (max 650 mg)
- Child > 6 months of age – Ibuprofen 10mg/kg PO x 1 (max 400 mg)
- Adult – Acetaminophen 650 mg PO x 1
- Adult – Ibuprofen 400 mg PO x 1
- FEVER: All patients who present to the ED Triage area will have their temperatures taken and documented in the electronic medical record. All patients who present with a temperature > 100.4º F (38º C) [can be axillary, rectal, or oral temperature] shall be offered acetaminophen or ibuprofen. If a previous antipyretic has been given (either at home or in triage), an alternate antipyretic will be given if temperature >100.4º F (38º C). Rectal temperatures must be obtained for all of the following pediatric patients: Infants less than 2 months old, Children less than 2 years old with the exception of children presenting with minor trauma, & Active seizure patients up to 3 years old
- DYSPEPSIA: Patients with a history of heartburn, gastritis, GERD, or dyspepsia or who complain of epigastric pain consistent with those conditions (e.g. burning epigastric pain that is relieved by food or antacids and worsened by spicy foods) shall be offered aluminum hydroxide and magnesium hydroxide antacid (Mag-Al Plus). Dosages shall be as follows:
- Child 3 – 11 years of age – 0.5 ml/kg (maximum 30ml)
- Child ≥ 12 years of age and Adult – 30ml PO
- NAUSEA: Patients with a complaint of nausea or vomiting will be offered Ondansetron orally. Dosages shall be as follows: Ondansetron ODT (oral disintegrating tab), oral solution, or IV form orally
- Child 6 months to 3 years of age – 2mg PO
- Child 4 – 11 years of age – 4mg PO
- Child 12 years of age to Adult – 4mg PO
- PAIN: All patients who arrive to the ED Triage area will have their level of pain assessed and documented in the EMR. The pain scales used are FLACC, Numeric, and Faces, depending upon the age of the patient. Dosages for fever and/or pain shall be as follows:
- Reassessment and Repeat Dosing
- Assessment of the patient’s symptoms (pain, fever, gastritis symptoms, nausea and/or vomiting) should be reassessed within 1 hours of the medication given in triage.
- Patients who after reassessment of pain (within one hour of receiving the 1st dose of acetaminophen or ibuprofen) continue to complain of pain and desire further analgesic treatment will then be offered acetaminophen or ibuprofen alternating from the previous medication administration.
- Patients who continue to complain of pain and/or fever may have a repeat dose of acetaminophen 4 hours after the initial dose, and/or a repeat dose of ibuprofen 6 hours after the initial dose.
- Patients who continue to complain of dyspepsia may have a repeat dose of aluminum hydroxide and magnesium hydroxide antacid (Mag-Al Plus) 6 hours after the initial dose.
- A nurse practitioner or physician provider will be notified of any patient that:
- The triage nurse assesses to require more analgesia than oral acetaminophen or ibuprofen or aluminum hydroxide and magnesium hydroxide antacid (Mag-Al Plus) can provide
- Develops any signs and/or symptoms of adverse reaction to acetaminophen, ibuprofen, aluminum hydroxide and magnesium hydroxide antacid (Mag-Al Plus), or ondansetron
- Any medication error that occurs shall be brought to the attention of the Attending overseeing the patient and the nurse who administered the medication. The patient and/or caretaker will be informed of the error. Standard procedures will be followed, as is the Department’s policy for other medication errors.
Approved November 2015, Chappell 2/22/16