Pelvic ultrasound (transvaginal)
Background

- Also known as endovaginal ultrasound
- Used to evaluate female reproductive organs including uterus, ovaries, fallopian tubes, cervix, and vagina
Indications
General
- Pelvic pain
- Abnormal pelvic or abdominal exam
Uterus
- Vaginal bleeding
- Fibroids
- IUD placement
Ovaries and adnexa
- Ovarian cyst
- Ovarian torsion
- Ovarian masses
- Tubo-ovarian abscess
- Hydrosalpinx
Pregnancy
- Confirm intrauterine pregnancy
- Gestational dating
- Fetal monitoring and surveillance
- Evaluation of placenta
- Spontaneous abortion
- Intrauterine fetal demise
- Ectopic pregnancy
- Heterotopic pregnancy
- Molar pregnancy
Technique
General
- Use 5 MHz endocavitary probe (high frequency, low penetration)
- Apply surgical lubricant inside and outside probe cover
- Place patient in lithotomy position
- Gently advance probe into vaginal canal and position adjacent to cervix
- May be more comfortable for patient to insert probe into vagina herself
- Apply gentle pressure to lower abdominal wall with one hand and manipulate probe with other hand
Longitudinal scan
- Probe marker pointing at 12:00
- Shows anterior structures on left side of screen
- Begin midline at endometrial stripe
- Scan from right to left through uterus
- Move probe laterally to view adnexa and ovaries
Transverse scan
- Rotate probe 90 degrees counterclockwise so probe marker is pointing at 9:00
- Shows right-sided structures on left side of screen
- Start at endometrial stripe and scan throughout uterus
- Locate cornual flare (junction of uterus and fallopian tubes)
- Move probe laterally along fallopian tube to locate ovary
- Ovaries identified by follicular (anechoic or hypoechoic) structures

Uterus in longitudinal plane

Cornual flare (uterus and fallopian tube junction) in transverse plane

Normal ovary with follicles



Normal Findings
Uterus
- Anteverted: Fundus pointing to anterior abdominal wall
- Retroverted: Fundus pointing to posterior wall
- Endometrial stripe: Measured from thickest echogenic area (from one basal endometrial interface to the other, including canal)
- Pre-menopausal:
- During menstruation: 2-4mm
- Early proliferative phase: 5-7mm
- Late proliferative phase: 11mm
- Secretory phase: 7-16mm
- After D&C or SAB: >5mm
- Consider retained POC if thicker
- Post-menopausal:
- With vaginal bleeding: <5mm
- Without vaginal bleeding: <11mm
- Pre-menopausal:

Normal thickened endometrial stripe during secretory phase

Normal thin endometrial stripe during menses


Ovaries
- Physiologic cysts present
- <3 cm diameter
- Ovarian follicle or corpus luteum
- Typically don't cause complications
Pregnancy (1st trimester)
- 4-5 weeks
- Gestational sac
- First sign of early pregnancy, usually seen between 3-5 weeks gestation
- "Double decidual sac" sign
- Two concentric rings (uterine lining and gestation lining) around anechoic gestational sac)
- Highly suggestive of intrauterine pregnancy (before yolk sac or embryo embryo visualized
- "Intradecidual sign"
- Thickened decidua on one side of uterine cavity surrounding anechoeic sac
- Gestational sac
- 5-6 weeks:
- Yolk Sac
- Circular (or sometimes as two parallel lines) echogenic structure with thick walls within gestational sac
- Definitive evidence of intrauterine pregnancy
- Multiple yolk sacs is earliest sign in multiple gestational pregnancy
- "Double bleb" sign
- Yolk sac and amniotic cavity that look like two bubbles within gestational sac
- Yolk Sac
- 6-7 weeks
- Fetal Pole
- First visual manifestation of fetus (or "embryo")
- Thickening of margin on yolk sac
- Cardiac activity present (FHR ~100-115 bpm)
- Crown rump length: ~5mm
- Fetal Pole
- 8-9 weeks
- Limb buds appear
- Head identifiable
- 9-10 weeks
- FHR ~170-180 bpm
- Fetal movement visible
- End of embryonic period
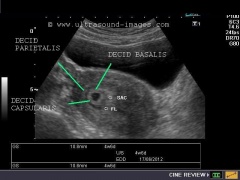
Double decidual sac sign
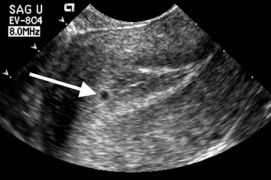
Intradecidual sign

Double bleb sign (yolk sac and amniotic cavity)

Fetal pole (Thickening of yolk sac on one side)




Abnormal Findings
Abnormal Pregnancy
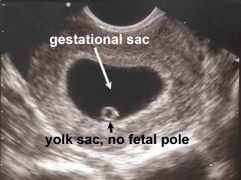
- Gestational sac >10mm without visible yolk sac
- Gestational sac >18mm without fetal pole
- Collapsed gestational sac
- Pseudogestational sac
- Endometrial breakdown during ectopic pregnancy
- May be erroneously interpreted as true gestational sac in ectopic pregnancy
- Irregularly shaped
- Located in endometrial cavity, instead of eccentrically within endometrium
- No yolk sac present
- May not have double decidual sac sign
- Absence of fetal heart beat in embryo with CRL >5mm
- FHR <90 bpm
- Molar pregnancy
- Many small, irregular cystic structures in endometrium
- "Snowstorm appearance"

Gestational sac greater than 10mm without yolk sac
Gestational sac greater than 18mm without fetal pole

Collapsed gestational sac

Pseudogestational sac
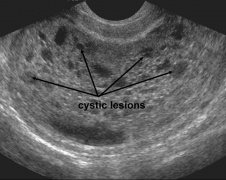
Molar pregnancy with multiple cystic lesions in endometrium ("snowstorm appearance")





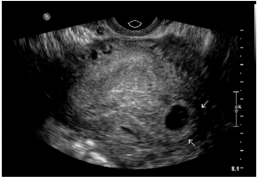
Ectopic pregnancy
- Implantation of blastocyst outside of endometrium
- Occur in fallopian tubes, cervix, ovaries, peritoneal cavity, or scar of prior uterine surgery
- Most definitive sonographic sign is gestational sac with yolk sac, embryo, or fetal heart beat outside of the endometrium
- Tubal pregnancy
- "Tubal ring" sign: echogenic thick-walled anechoic sac visualized between uterus and ovary (separate from ovary when pressure applied to fallopian tube with probe)
- Interstitial Pregnancy
- Implantation of gestational sac in muscular wall of uterus at proximal regional of fallopian tubes
- "Interstitial line" sign: hyperechoic line from endometrial stripe to cornual region adjacent to interstitial gestational sac
- Cervical Pregnancy
- Implantation of gestational sac below internal cervical os
- Can cause life-threatening hemorrhage
- Must distinguish between cervical ectopic and spontaneous abortion at level of cervix:
| Cervical ectopic | Spontaneous abortion at cervix |
| Hour-glass shaped uterus | Elongated gestational sac |
| Gestational sac with yolk sac, fetal pole, or heartbeat | Absent embryonic cardiac activity |
| Closed internal os | Dilated internal os |
| Color doppler showing hypervascular trophoblastic ring | Sac moves in cervix with gentle probing (“Sliding sac sign”) |
| Empty uterine cavity | Loss of sac on serial imaging |
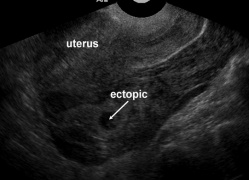
Ectopic pregnancy

Free fluid in cul-de-sac with no gestational sac visualized in uterus
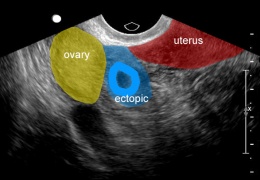
Ectopic pregnancy between ovary and uterus, suggestive of tubal ectopic
Interstitial pregnancy
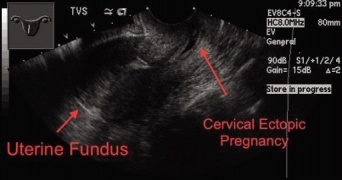
Cervical pregnancy





Ovarian Torsion
- Bimodal age distribution: young women (15-30yo) and post-menopausal women
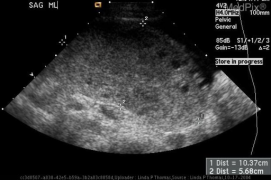
- Typically occur in enlarged ovaries (>5cm)
- Benign mature cystic teratomas
- Hemorrhagic/large ovarian cysts
- Cystic neoplasms
- Cystadenomas
- Polycystic ovarian syndrome
- Sonographic signs associated with torsion
- Enlarged ovary from edema, engorgement, hemorrhage
- Midline ovary
- Free pelvic fluid
- Underlying ovarian lesions
- Peripherally displaced follicular cysts
- Doppler findings:
- Decreased/absent venous or arterial flow
- Absent/reversed diastolic flow
- Can have normal flow (from dual supply from uterine and ovarian arteries)
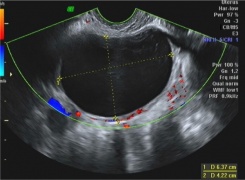
Large ovarian cystadenoma

Hemorrhagic ovarian cyst with blood clot
Large midline ovary with multiple peripherally located follicular cysts (torsion)
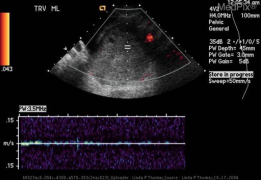
Absent color doppler and venous and arterial waveforms (torsion)




Pearls and Pitfalls
- Free pelvic fluid with positive hCG is ectopic pregnancy until proven otherwise
- Presence of doppler flow cannot rule out ovarian torsion
Documentation
Normal Exam
Abnormal Exam
Clips
External Links
See Also
References
- www.radiopaedia.org
- www.acep.org/sonoguide
- www.fetalultrasound.com