Periorbital swelling
Background


- This page describes a general approach to the complaint of periorbital swelling[1][2]
- The critical EM distinction is preseptal (periorbital) cellulitis vs. orbital cellulitis
- The orbital septum is the key anatomic landmark separating the two
- Preseptal cellulitis: infection anterior to the orbital septum — common, usually manageable outpatient
- Orbital cellulitis: infection posterior to the orbital septum — emergency with vision-threatening and life-threatening complications
- Other important causes include allergic reactions, insect stings, angioedema, and nephrotic syndrome
Clinical Features
History
- Onset: acute (hours — allergic, infectious, trauma) vs. gradual (days — cellulitis, systemic)
- Unilateral vs. bilateral:
- Unilateral: more likely infectious (cellulitis, dacryocystitis), traumatic, or insect sting
- Bilateral: more likely systemic (allergic, nephrotic syndrome, thyroid disease, SVC syndrome)
- Recent sinus symptoms (sinusitis is the most common cause of orbital cellulitis)
- Recent trauma, insect bite/sting, skin break
- Fever (infection)
- Pain, particularly with eye movement (orbital cellulitis)
- Vision changes, diplopia (orbital cellulitis — concerning for optic nerve compression)
- Dental pain or recent dental procedure (odontogenic source)
- Allergic history, medication changes
Physical Exam
- Extent and distribution of swelling (unilateral vs. bilateral, periorbital vs. diffuse face)
- Erythema, warmth, tenderness
- Key findings distinguishing orbital from preseptal cellulitis:
- Pain with extraocular movements (orbital)
- Proptosis (orbital)
- Decreased visual acuity (orbital)
- Ophthalmoplegia / limited extraocular movements (orbital)
- Afferent pupillary defect (orbital — suggests optic nerve involvement)
- Chemosis (orbital)
- Palpate for fluctuance (abscess)
- Examine for dacryocystitis (medial canthal swelling, expressible purulence from punctum)
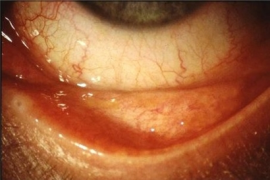
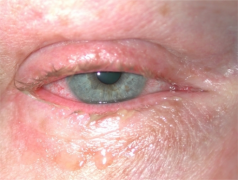
Periorbital swelling images

Blepharitis of eyelashes.

Infant Blepharitis (right)

Bilateral dacryoadenitis

External stye

Internal stye
Acute allergic conjunctivitis
Chronic allergic conjunctivitis

Contact blepharoconjunctivitis

Proptosis due to retrobulbar abscess and orbital cellulitis















Red Flags
- Pain with eye movement → orbital cellulitis
- Decreased visual acuity → optic nerve compromise
- Proptosis → retrobulbar process
- Bilateral periorbital edema in child → nephrotic syndrome
- Periorbital swelling + lip/tongue swelling + dyspnea → angioedema / anaphylaxis
- Fever + periorbital swelling + altered mental status → cavernous sinus thrombosis
Differential Diagnosis
Periorbital swelling
Proptosis
- Normal IOP
- Orbital cellulitis
- Orbital pseudotumor
- Orbital tumor
- Increased IOP
- Retrobulbar abscess
- Retrobulbar emphysema
- Retrobulbar hemorrhage
- Ocular compartment syndrome
- Orbital tumor
No proptosis
- Periorbital cellulitis/erysipelas
- Dacryocystitis (lacrimal duct)
- Dacryocele/Dacryocystocele
- Dacryostenosis
- Dacryoadenitis (lacrimal gland)
- Allergic reaction
- Nephrotic Syndrome (pediatrics)
Lid Complications
- Blepharitis (crusts)
- Chalazion (meibomian gland)
- Stye (hordeolum) (eyelash folicle)
Other
- Subperiosteal abscess
- Orbital abscess
- Cavernous sinus thrombosis
- Conjunctivitis
- Contact dermatitis
- Herpes zoster
- Herpes simplex
- Sarcoidosis
- Granulomatosis with polyangiitis
Infectious
- Preseptal cellulitis (most common infectious cause)
- Orbital cellulitis (emergency — often from adjacent sinusitis)
- Dacryocystitis (medial canthal swelling)
- Hordeolum/chalazion (focal eyelid swelling)
- Herpes zoster ophthalmicus (V1 distribution)
Allergic/Inflammatory
- Allergic reaction / angioedema
- Insect bite/sting
- Contact dermatitis
- Idiopathic orbital inflammation (orbital pseudotumor)
Systemic
- Nephrotic syndrome (bilateral periorbital edema, often worse in morning)
- Hypothyroidism (myxedema)
- Superior vena cava syndrome
- Heart failure
Traumatic
- Blunt trauma / periorbital hematoma
- Orbital fracture with subcutaneous emphysema
- Subperiosteal hematoma
Evaluation
Bedside
- Visual acuity (each eye)
- Pupillary exam (RAPD)
- Extraocular movements
- IOP if proptosis present
Laboratory
- CBC with differential if infection suspected
- Blood cultures if febrile or toxic-appearing
- UA with urine protein, BMP, albumin if bilateral edema and nephrotic syndrome suspected
- ESR, CRP for inflammatory markers
Imaging
- CT orbits with contrast (with thin cuts through sinuses): gold standard for distinguishing orbital from preseptal cellulitis
- Evaluates for orbital abscess, subperiosteal abscess, sinusitis, and cavernous sinus
- CT should be obtained whenever orbital cellulitis is suspected
- MRI/MRV if cavernous sinus thrombosis suspected
Management
Preseptal Cellulitis
- Outpatient oral antibiotics in most cases: amoxicillin-clavulanate or clindamycin
- Warm compresses
- Close follow-up in 24-48 hours
- IV antibiotics if: young child (<1 year), unable to take oral, toxic-appearing, failed outpatient therapy
Orbital Cellulitis
- Admit for IV antibiotics: vancomycin + ceftriaxone (or ampicillin-sulbactam + vancomycin)
- ENT and ophthalmology consultation
- Surgical drainage for subperiosteal or orbital abscess if meeting criteria (large abscess, no improvement with IV antibiotics, vision compromise)
- Monitor visual acuity serially
Allergic/Angioedema
- Antihistamines (diphenhydramine, cetirizine)
- Epinephrine if anaphylaxis or airway compromise
- See Angioedema for specific management
Dacryocystitis
- Warm compresses, oral antibiotics (amoxicillin-clavulanate)
- Ophthalmology referral for recurrent cases (may need dacryocystorhinostomy)
- IV antibiotics if severe/periorbital spread
Disposition
Admit
- Orbital cellulitis
- Preseptal cellulitis in young infants or immunocompromised
- Cavernous sinus thrombosis
- Angioedema with airway concern
Discharge
- Uncomplicated preseptal cellulitis with oral antibiotics and 24-48 hour follow-up
- Allergic periorbital swelling responding to antihistamines
- Insect bite/sting without systemic reaction
- Return precautions: worsening swelling, vision changes, pain with eye movement, fever, difficulty breathing
See Also
Eye Algorithms
- Red eye
- Periorbital swelling
- Acute vision loss (noninflamed)
- Acute onset flashers and floaters
- Painful eyes with normal exam
- Neonatal eye problems