OVMC:ED
All information previously published on this page is now hosted at Olive View Medical Center on Microsoft OneNote. You can access it from any LADHS computer using your DHS credentials and the link above.
WikEM OVMC:ED is meant as a guide to providers working in the ED at Oliveview UCLA Medical Center. It is only a guide. Management of the patient is always at the discretion of the ED provider.
Know Your Rights (Immigration Rights)
- Link below to DHS "Red Cards" (immigrant rights) in 20 different languages
OOP/non-DHS Patients referred to OVMC for Specialty Care
HIPAA compliant link https://forms.office.com/g/Gr8EEkMiGW
OVMC Observed Procedure Checklist and Evaluation Form
Procedure Checklist and Evaluation Form
OVMC Administration Master Phone List
OVMC Administration Master List
DEM Master Backup Supply List
Phone Numbers
ED
- MD Room ED 1A Attendings 73648, 73649
- MD Room ED 1A Residents 73907, 74732, 73645, 74720 (phones running in direction of ED1 to ED2)
- MD Room ED 4/5 74936, 74937, 74938, 74939
- Hospitalist Room 74930
- ED 1A/Clerk: 74324 (PR1,PR2,15,24,25)
- ED 1B: 74865 (16-23)
- ED 2A: 74321 (1-7)
- ED 2B: 74280 (8-14)
- ED 3: 74976 (43-49)
- ED 4/RME Unit: 74974 (34-41)
- ED 5: 74970 (26-33)
- ED Fax: 74298
- Charge/Resource Nurse: 74324
- ICN/Router: 73440
- Triage 1: 65658
- Triage 2: 65661
- Triage 3: 65662
- RME 1: 73789
- RME 2:
- Triage 7: 75709
- ED Lab 74977
- ED Xray tech 74951
- ED CT scan tech 74968
- ED Ultrasound tech 74940, 74945
- ED Reading Room 74969, 74971
- ED Pharmacy 75011
- Psych ED 74340, 74341
- UR 74890, 74891
- PFS 65228
- TFU 74825
- ED North Annex 73107
Translator Phones in Room
- PR 1 x60400
- PR 2 x60401
- Bay 1 x60346
- Bay 2 x60347
- Bay 3 x60348
- Bay 4 x60349
- Bay 5 x60350
- Bay 6 x60351
- Bay 7 x60352
- Exam Rm 8 x60353
- Exam Rm 9 x60354
- Exam Rm 10 x60355
- Exam Rm 11 x60356
- Exam Rm 12 x60357
- Exam Rm 13 x60358
- Exam Rm 14 x60359
- Exam Rm 15 x60360
- Exam Rm 16 x60361
- Exam Rm 17 x60362
- Exam Rm 18 x60363
- Exam Rm 19 x60364
- Exam Rm 20 x60365
- Exam Rm 21 x60366
- Exam Rm 22 x60367
- Exam Rm 23 x60368
- Exam Rm 24 x60369
- Exam Rm 25 x60370
- Exam Rm 26 x60371
- Exam Rm 27 x60372
- Exam Rm 28 x60373
- Exam Rm 29 x60374
- Exam Rm 30 x60375
- Exam Rm 31 x60376
- Exam Rm 32 x60377
- Exam Rm 33 x60378
- Exam Rm 34 x60379
- Exam Rm 35 x60380
- Exam Rm 36 x60381
- Exam Rm 37 x60382
- Exam Rm 38 x60383
- Exam Rm 39 x60384
- Exam Rm 40 x60385
- Exam Rm 41 x60386
- Exam Rm 42 x60387
- Exam Rm 43 x60388
- Exam Rm 44 x60389
- Exam Rm 45 x60390
- Exam Rm 46 x60391
- Exam Rm 47 x60392
- Exam Rm 48 x60393
- Exam RM 49 x60394
Anesthesiology/Airway
- Pager: 818-529-0372
- VOIP Phone: 75112
Psych ED
- Psych ED Front Desk 74340
- Psych ED Doctor Room 73950
Inpatient
- ICU
Radiology Techs
- Main Radiology 74059
- ED Xray tech 74951
- ED CT scan tech 74968
- ED Ultrasound tech 74940
- ED Reading Room 74971
- MRI tech 73862
- MRI front desk 73535
- Interventional Radiology Scheduling 73686
Radiology Reading Rooms
- ED Reading 74971
- MRI Body Reading 73770
- Neuro and MRI Neuro Reading 74082
- MSK/General Reading 65145
- UTZ Reading 74177
- CT Reading 74791, 74792, 66078
- Interventional Radiology 74554
- Overnight read hours: Monday-Friday 11pm-7am, Sat/Sun/Holidays 7pm-7am
- Overnight Reads: USROC (utz, plain films) 866-448-7762
- Overnight Reads: StatRad 858-546-3800
- On-call schedules for Radiologists and Tech Supervisor: https://lacounty.sharepoint.com/sites/dhs-ov-radiology/Radiology%20On%20Call%20Schedules/Forms/AllItems.aspx
Lab
- Lab - ED Phlebotomy 74977, 74978
- Lab - Processing 66033
- Lab - Results 66033
- Lab - Blood Gas 73314
- Lab - Micro 66045
- Lab - Pathology 73532
- Lab - Blood Bank 74062
Pharmacy
- ED Pharmacist 75011
- ED Pharmacist lives in fishbowl near Radiology
- Pharmacy Outpt 73070
- Monday - Friday 7:30am-8:00pm; Sat, Sun, Holidays 8:30am-4:30pm
- Prescription drop-off times: Mon-Friday until 6:30pm; Sat, Sun, Holidays until XXX
- Eprescribing "cut-off" times: Mon-Friday 7:00pm; Sat, Sun, Holidays 3:30pm
- Pharmacy Inpt 73059, 573061
- EPCS Electronic Prescribing of Controlled Substances
Respiratory Therapy
- RT Supervisor 75038
- DEM RT 75581
- RT Lead Therapist 75331
- RT Pager 818-542-1156
Nursing
- ED Charge Nurse/Throughput RN in ED1A 75333
- ICN/Router: 75235, 75236
- ED Nursing Supervisor Office (near bed #8) 74850
- Triage 1: 75658
- Triage 2: 75661
- Triage 3: 75662
- Triage 4/RME: 75697
- ED 1A/Clerk: 74323, 74324
- ED 1B: 74865
- ED 2A: 74321
- ED 2B: 74280
- ED 3: 74976
- ED 4/RME Unit: 74974
- ED 5: 74970
- Hospital Nursing Administration 73001
Clinics
| Urgent Care Clinic and CCC 2A105 74312 | Open Mon-Sat |
| Clinic A 73125 | |
| Clinic B 73129, 73131, 73132 | Breast, Chest, Gen Surg, Peds Urology, Plastic Hand, Plastic Surg, Proctology, Thoracic Surg, Urology, Vasc Surg |
| Clinic C 73133 | Primary Care, GI, HIV/Positive Health, Cardio, Heme, ID, MDA, Neuro, Oncology |
| Clinic D 73137 | Gyn After Care, Gyn, Gyn Onc, Urogyn, Gyn Endo, Memory |
| Clinic E 73064 | ENT, Interventional Rads, Ortho, Podiatry, Rheum |
| Clinic M 74546 | Respiratory Urgent Care |
| Clinic P 73700 | Primary Care, Derm, Endo, Pulm, Renal, Women's Health |
| Ophtho 75630 | |
| Peds Clinic in 4C 73144 | |
| Ortho Tech 818-529-5135, 818-529-5509 |
Operator
- "0" then "5" then "5"
Other
- ANO 75526
- Appointment Center 747-210-8000
- Bed Control 75959, 73179
- Central Supply 65946
- IT Info Technology 74522, 72644, 323-409-8000
- OR 74364
- PFS (Patient Financial Screening/Registration) 65228
- Medical Administration 73025
- Medical Records (problems with Cerner notes) 73934
- Physical Therapy 74245, room 1D120
- Psych ED 74340, 74341
- Resp Therapy RT office 74422, pager 4055...1392...enter callback number
- Sheriff
- Social Work 74236
- Social Work pager 818-313-1759
- Social Work after hours for emergencies like deaths, 818-313-1637
- SUD Counselor 74773
LA General
- ED Resusc 323-409-6667
- ED Resusc Attending 323-409-1610
- ED Peds Attending 323-409-1650
MAC
- 866-940-4401; press "1" for emergent, or press "3" for DHS facility
Kaiser EPRP
- 800-447-3777
ED Administration
ED Admin Gurus
- Matt - Neurology, Neurosurgery, Infection Control, EMS, and Disaster
- Pam - Ob/gyn
- Maureen - Pediatrics, Substance Use Disorders
- Alan - Radiology
- Fred - Psych
- Amir - Medicine and ICU
- Tomer - Pharmacy and P&T (pharmacy and therapeutics committee)
- Breena - IRB, Invasive Procedures and Language assistance (interpreter issues, video phone issues…)
- Steven - Residency
- Kellie - Residency
- Luis - Cerner
ED In Person Translation Service for Hard of Hearing, Deaf, Deaf Blind, non-ASL speakers
- see Social Work section
ED Throughput
RME Unit
- Monday - Sunday, 8am to 8pm
- ED 4: 34,35,36,37,38,39,40,41
- ED 31/Procedure/Discharge Room will be left open and used for slit lamp exams and ENT procedures as needed, consults and discharge patients home as needed.
- Staffing: two NPs, two RNs, one NA
- Responsible for ESI level 4 and 5 patients
- Responsible for overall turnover of rooms by discharging patients and bringing in new patients to be seen
- NP and RN will pair up and take 4 rooms each, 34-37 and 38-41
- RME Unit rooms will be set up with gurney against the wall and a chair in center of room in which patients will be placed.
- Patients who remain in the ED 4 from the nightshift will either be discharged or moved to another area as soon as is possible for nursing staff. Night shift staff will attempt to move these patients at 6am. Dayshift stay will continue moving patients held over from the night shift.
- In the morning when ED 4/RME Unit rooms are empty, Triage RN will place ESI level 4 or 5 patients directly into empty ED 4/RME Unit rooms; when these rooms are finally full, the responsibility for room turnover will shift to the staff in the RME Unit.
- In the morning, when ED 4/RME Unit beds have been filled by the Triage RN, additional ESI 4 and 5 patients can continue to be placed into other ED beds in ED 1,2,3 or 5 if ESI 1-3 patients do not take precedent.
- NP provider will sign up for the patient in the Res/ML column
- RN will not sign up for the patient on the Tracking Board. The RN, however, will be responsible for patients who are under the care of the NP with which they are paired.
- RN is not required to complete an assessment on every RME Unit patient. If medications given, etc, then a reassessment should be completed. If RME Unit patients are on the track more than 4 hours, a reassessment must be done by the RME Unit RN in the waiting room.
- RME Unit Nursing (RN/NA) responsibilities: visual acuities, drawing blood, obtaining urine samples, sending patients needing plain films to PWR, calling Radiology about patients need utz or CT scan, anticipating procedures such as lac repairs or gyn exams and moving carts to the room, moving patients to and retrieving patients from the waiting room, etc.
- Any patient placed in RME Unit who is subsequently deemed too complicated for RME Unit will have an RME documented, their ESI level changed to 3, orders placed as needed, and patient moved either back to the waiting room or when possible to ED 1, 2, 3, or 5. Responsibility for these patients should also move to the ED provider and nursing staff in those areas. If moved back to the waiting room, responsibility falls back to the Triage and Reassessment RNs.
- Patients requiring plain films will be sent down to PWR/Radiology WR to wait for their imaging. RN or Provider will change the bed assignment to PWR. Radiology tech will then look on the tracking board, find the patient in PWR, complete the plain film imaging and then tell the patient to return to the RME Unit/ED 4 Nursing Station. The RME Unit RNs will then change the bed assignment to TR4 and send patient to waiting room to wait for imaging results.
- ONLY RME Unit patients requiring plain films will be sent to PWR/Radiology WR.
- Patients who are waiting for laboratory testing results, imaging such as utz or CT, plain film imaging results, or consultations by subspecialits can be moved to the waiting room. Bed assignment will be changed to TR4 in order to keep them visually separate from the other waiting room patients. These patients will remain the responsibility of their providers while they are in the WR awaiting results.
- Patients moved to the waiting room (TR4) or ED 31/Procedure/Discharge Room will not be counted toward the nurse/patient ratios because they will need limited nursing interventions.
- Patients who need to receive discharge instructions will be discharged in their ED room assigned or in ED 31/Procedure/Discharge Room.
- RN will notify housekeeping when a room needs to be cleaned; RN will choose a new ESI level 4 or 5 patient from the WR to fill the room.
- At 7pm the night shift RNs assigned to RME Unit will assume care for the day shift RN’s patients and continue working with the NP per the above guidelines.
- At 8pm, the RME Unit will close, and patients who are still in progress of being cared for by the RME Unit team will be signed out by the day shift NPs to one of the night shift residents. The night shift RNs assigned to EDs 4 continue to care for the patient until discharge.
- At 8pm, ED 4 will be used along with ED 1,2,3 and 5 beds for a variety of patients. Triage RN will be responsible for assigning patients to those beds.
- If the RME Unit is successful, we may extend hours to 8pm-8am when a night shift Nurse Practitioner has been hired. We may also extend the RME Unit, as needed, to include additional ED beds and other ED nursing and provider staff.
Nursing
MIT Meds in Triage
- Triage RNs are able to administer acetaminophen, ibuprofen, ondansetron or mylanta under a Medication in Triage Protocol
- Applies to adults and children
- One time dose only
- If patient has already been RME'd and requests pain medication, then MIT protocol does not apply and provider will be asked to order medication
Admission Guidelines
Medicine Admissions UPDATE March 2017
- ED Provider contacts Hospitalist and discusses case (ONE PHONE CALL)
- Hospitalist has one hour to see patient and obs vs admit, level of care, admission team
- If hospitalist desires discharge or transfer, hospitalist will recontact ED providers and discuss
- Hospitalist will place order for Request for Admit (Red circle)
- Hospitalist will contact the Admitting Team and tell them about the case
- Admitting Team will write inpatient Admission Orders (Hospital icon)
- If Admitting Team desires more information, Admitting Team will contact ED provider
Medicine Admissions Upgrades, Downgrades, ICU Admits co-managed
- Inpatient teams are required to write inpatient admission orders (hosp icon) within 2 hours of Order to Admit (red circle)
- Once inpatient admission orders are written (hosp icon),both Attending and Resident column on Tracking board can be changed to Inpatient Attending and Inpatient Resident
- ED Admissions to Ward, Tele, Stepdown are managed by inpatient Medicine team once hospital icon appears
- ED Admissions to ICU are managed by ED with ICU consultation
- Ward, Tele, Stepdown then upgraded to ICU are co-managed by original medicine inpatient service and ICU team
- ICU then downgraded to Ward, Tele, Stepdown are managed by the inpatient medicine team; ED should give report to Medicine
Observation - updated May 28, 2021
- We can page hospitalist for Obs admissions or overrides up to 11pm.
- If we have a patient who is still in interqual process and/or still awaiting some parts of the workup, but for whom we already know they will not be going home, we should contact the hospitalist before 11pm. With discussion, they can be put on the list for the Night Admitting Resident to be admitted or placed in Obs after 11pm. The goal is to allow discussion with hospitalist before ED resident and attending signout to the overnight ED team. (Most of the time we should wait until we have the essential workup done to call the hospitalist)
- DEM will continue to keep patients who do not meet interqual in the ED overnight and manage them. We will NOT place the Obs order on these patients, and they will remain under ED care. Put a "ED OBS" comment in the MD column so we can identify them.
- In the morning those who cannot be discharged within a few hours should be discussed with the hospitalist for override or Obs placement under medicine. It's a good idea for the overnight attending to call the hospitalist around 7:15 to discuss them before signout, if the hospitalist has not already called or come by.
Chest Pain Admission Guidelines
- High Risk = Any of the following:
- Objective signs of myocardial infarction/ischemia or new LV dysfunction:
- Diagnostic ST/T changes or new LBBB on EKG
- Abnormal Troponin result
- Symptoms associated with dynamic EKG changes
- Signs of CHF or cardiogenic shock
- Malignant dysrhythmias
- Typical symptoms known to be ischemic and:
- Recent (<12 month) PCI
- Recurrent/refractory despite anti‐anginal therapy
- Management:
- Anti‐platelet, anti‐thrombotic, and anti‐anginal therapy
- Cardiology consult for possible urgent invasive therapy
- Repeat troponin q3h x3 unless urgent invasive therapy already planned
- Admit to SDU or ICU bed
- Objective signs of myocardial infarction/ischemia or new LV dysfunction:
- Intermediate Risk = No High Risk Features, but one or more of the following:
- Abnormal but non‐diagnostic EKG, cannot exclude ischemia:
- LVH with strain
- Digoxin effect
- Ventricular‐paced rhythm
- New, typical angina symptoms in a patient with:
- Known CAD
- Age>70
- Inability to complete outpatient ETT
- Intermediate Score on Risk Estimation Tool (e.g., TIMI 3 or higher)
- Management:
- ASA; anti‐anginal therapy as needed
- Repeat EKG and troponin q3h until negative assay >6h from onset of most recent chest pain
- Observation or Telemetry admit (in consultation with Hospitalist and/or Cardiologist) for risk stratification prior to discharge, unless already performed in past 12 months.
- Abnormal but non‐diagnostic EKG, cannot exclude ischemia:
- Low Risk = No High or Intermediate Risk feature, plus
- TIMI 0-2
- Highly atypical symptoms
- Recent negative objective study (e.g. angiogram, nuclear imaging, CCTA, ETT with Duke score 9 or greater)
- Management:
- ASA
- Repeat EKG and troponin q3h until negative assay >6h from onset of most recent chest pain
- Refer for expedited (<72h) outpt. risk stratification if not already done in past 12 months
- Refer for primary care to assess and manage vascular risk factors
Tele Admission Guidelines
- Based on AHA/ACC guidelines, see reference at: http://circ.ahajournals.org/content/110/17/2721.full
- Class I (Valid for 72 hours)
- CONSIDER SDU OR ICU LEVEL OF CARE, IF INDICATED
- Mild – moderate heart failure (Requiring IV Diuretics BID, not PRN)
- Hemodynamically stable arrhythmia (HR > 45 and < 150 bpm):
- atrial fibrillation/flutter
- non-sustained ventricular tachycardia
- other non-sustained SVT
- Following percutaneous coronary intervention (PCI)/cardiac cath
- QTc prolongation (> 460 msec in women, > 450 msec in men)
- Hemodynamically stable (HR > 45 bpm) atrioventricular block (consider higher level of care for 3rd deg)
- Drug overdose with arrhythmic potential (e.g. Digitalis, Tricyclic antidepressants, Phenothiazines, Antiarrythmics)
- Class II (Valid for 48 hours):
- Transfer from ICU or SDU after Acute Coronary Syndrome (STEMI/NSTEMI) or cardiac/respiratory arrest
- Chest pain requiring inpatient evaluation (troponin < 0.8, no significant ECG changes)
- Stroke
- Syncope (true loss of consciousness)
- Post-operative patients with presumptive or confirmed obstructive sleep apnea
- Cardiac contusion, myocarditis or pericarditis
- Initiation/adjustment of antiarrhythmic medications
- Class III (Valid for 24 hours):
- Electrolyte abnormality requiring cardiac monitoring but not requiring higher level of care due to underlying process such as diabetic ketoacidosis
- Following pacemaker placement or cardioversion
- Asthma/COPD exacerbation with hypoxemia (spO2 less than or equal to 95%) despite high flow O2 treatment
Surgical Subspecialty Admission Guidelines
- DATE: February 14, 2023
- TO: Faculty and Housestaff, Departments of Surgery, Medicine, Ob/Gyn, Pediatrics, and Emergency Medicine
- FROM: Jane Yang, M.D., Interim Chief, Department of Surgery; Soma Wali, M.D., Chief, Department of Medicine; Christine Holschneider, MD, Chief, Department of Obstetrics & Gynecology; Shannon Thyne, MD, Chief, Department of Pediatrics; Greg Moran, M.D., Chief, Department of Emergency Medicine
- Re: Emergency Department Hospital Admission Guidelines: IIn order to optimize patient care, housestaff supervision, expedite the admission process, and minimize conflicts regarding admission decisions, this document will clarify how the decision is made to admit emergency department (ED) patients to various inpatient services, and provide guidelines as to what types of patient diagnoses are most appropriately admitted to a specific inpatient service and hospital ward or unit.
- Decision to Admit an ED Patient to the Hospital & Resolving Disputes: The decision as to whether a patient can be managed as an outpatient or requires more intensive observation and therapy in the hospital can be critically important. Therefore, the service chiefs have decided that after input from the admitting housestaff, the decision regarding admission ultimately must be made by attending physicians, which is consistent with community standards of care.
- The Department of Emergency Medicine attending physician will make the decision on the need for an ED patient to be admitted. This decision will be made after reasonable evaluation and consultation to determine a presumptive diagnosis, admission service, and level of care. To avoid misunderstandings and delays, consulting residents should, upon completing their evaluation, clearly communicate their recommendations with the ED resident caring for the patient prior to leaving the ED. Patients will not be transferred from the ED to the floor until there is notification and confirmed acceptance by the admitting resident or attending, which should be indicated in the ED patient tracking system.
- If, once notified, the admitting service resident disagrees with the recommendation of the ED staff, the resident should contact his/her senior/chief resident or attending physician to review the case. All disputes should be resolved first by ED resident discussion with the admitting service senior/chief resident, and, if necessary, by discussion between the ED and the admitting service attending physicians.
- Diagnosis-Specific Guidelines for Appropriate Admission Service
- The service chiefs expect that patients with certain designated illnesses will be admitted to the appropriate service, in accordance with the preceding section. Patients with disorders appropriate for surgical admission may not require an acute surgical procedure (e.g., abdominal pain with possible ischemic bowel admitted for observation). Patients with potential surgical diagnoses but who have significant concomitant medical problems (e.g., diabetes out-of-control) may be best managed on the Medicine service, with close consultation.
- For patients seen in the ED who are within 30-days from their operation and for whom admission is being considered, the operative service (general surgery, urology, GYN, etc) should be the primary consulting service and in most cases the admitting service.
| General Surgery & Subspecialties | Medicine/Pediatrics/Ob/Gyn |
| Acute abdominal pain - very likely underlying surgical etiology (e.g., ischemic bowel), complicated diverticulitis likely to require surgery - non-pregnant (General Surgery) | Acute abdominal pain – unclear but possible medical/ non-surgical etiology (e.g., colitits, gastroparesis, uncomplicated diverticulitis) (Medicine) |
| Pregnant women and non-pregnant women with acute abdominal pain likely to have gynecologic etiology (Ob/Gyn with General Surgery consultation) | |
| Acute cholecystitis, Cholangitis, Choledocholithiasis in patient with gallbladder, symptomatic biliary colic with PO intolerance (General Surgery) | Gallstone pancreatitis in patient with or without a gallbladder, Alcoholic and other non-gallstone-related pancreatitis, Choledocholithiasis without gallbladder (Medicine) |
| Pregnant women with gallstone pancreatitis, acute cholecystitis, choledocholithiasis/cholangitis (Ob with General Surgery consultation) | |
| Hepatitis and hepatic abscess(es) (Medicine) | |
| Mechanical small bowel obstruction requiring NG tube (General Surgery) | Small bowel obstruction – secondary to prior Ob/Gyn surgery or gynecologic malignancy (Ob/Gyn) |
| SBO not requiring NG tube, or if not surgical candidate – (Medicine) | |
| Abscesses with complex wounds or requiring urgent OR intervention, necrotizing skin and soft tissue infections, post-operative wound infections, other significant skin/soft tissue infections involving specific areas needing urgent surgery (General Surgery, Head & Neck Surgery, Plastic Surgery for hand) | Cellulitis/lymphangitis, abscesses that do not require urgent OR intervention, and other skin infections with significant concomitant medical problems (e.g., diabetes out-of-control) (Medicine with surgical consult as needed); Infection of lower leg below ankle or foot with or without abscess, including diabetic foot ulcer and/or osteomyelitis (Medicine with Podiatry consultation) |
| Vulvar abscess (Gyn); | |
| Infection of lower leg below ankle or foot with or without abscess, including diabetic foot ulcer and/or osteomyelitis (Medicine with Podiatry consultation) | |
| Kidney stones with uncontrollable pain, with or without obstruction, without infection; Bilateral hydronephrosis from ureteral stones and renal insufficiency or solitary kidney; Acute prostatitis, with severe obstructive voiding symptoms, or with severe hydronephrosis; Scrotal abscess requiring OR intervention (Urology) | Urinary tract infection (Medicine), UTI with pregnancy (OB) or UTI with gynecologic malignancy (Gyn) |
| UTI requiring admission, with kidney stone or indwelling ureteral stent, with or without obstruction | |
| Acute prostatitis (fever, chills, toxic appearing); | |
| Epididymitis requiring admission for IV antibiotics; | |
| Scrotal abscess not requiring OR but needs IV abx; | |
| Urologic problem in patient with any complicated medical problem (e.g., diabetes out of control, severe sepsis) (Medicine with Urology consultation); pregnancy (OB), or gynecologic malignancy (Gyn) | |
| Acute gastrointestinal bleeding (Medicine or Pediatrics) | |
| Injuries distal to the elbow requiring urgent operation (Plastic Surgery) | Ankle and foot fractures (Medicine with Podiatry consultation) |
| All patients with post-operative surgical problems within 15 days of discharge requiring admission - to specific operating service (with Medicine consultation as necessary) |
- Admission Orders Admission orders must be written by the responsible inpatient service housestaff who are available to floor nursing in order to direct inpatient management.
- For cases in which the admitting diagnosis is established (e.g., CT-confirmed appendicitis), an inpatient bed is available, and the admitting service residents are unavailable for > 2 hours (e.g., in the OR), the ED resident will contact the admitting service senior/chief resident in order to seek verbal approval for the admission. The ED physician will then write holding admission orders on the standard admit form and transfer the patient to a hospital bed.
- If the admitting senior/chief resident is also unavailable or the admission cannot be approved, then the ED attending may contact the admitting service attending physician to facilitate the admission. Admission holding orders should include pain medications, intravenous fluids, and antibiotics (if recommended by the admitting service), and contact information (resident name and pager number) for the admitting service if a nurse needs new orders or to notify a physician about any change in patient status
- Patient Transfers
- All patients considered for transfer from Olive View-UCLA must be reviewed and evaluated by the ED attending physician.
- For pediatric patients, the pediatric attending physician on-call should be notified prior to patient transfer.
- For surgical diagnoses the attending surgeon on-call should be notified to approve the transfer.
- Admission Orders Admission orders must be written by the responsible inpatient service housestaff who are available to floor nursing in order to direct inpatient management.
Admissions from the Clinic, How to
- Clinic staff places order for "UR Consult"
- Once UR approves admission through Interqual, UR will contact PFS for a new FIN number to be created
- UR will then fax admission info and new FIN number to Bed Control
- Bed Control then contacts clinic staff to give them the new FIN number so admission orders can be placed
- Clinic staff or inpatient team must write Admission Orders in order for Bed Control to secure a bed
- For admissions to Obs Unit, clinic staff should contact Hospitalist on-call
Follow Up Guidelines
Future OVMC Clinic Appointments already scheduled
- Future OVMC appointments can be found in the Patient's Chart, tabs on the left, Patient Schedule
- Future OVMC appointments can also be found on the Patient Summary (Discharge Instructions). Click Depart. Page that appears is the Patient Summary. Scroll down to Future Appointments.
Future Orders - Outpatient studies ordered by the ED
- When you order a future outpatient study, it will automatically print on the Patient Summary (discharge instructions)
- Phone numbers for Radiology, Cardiology Lab and TFU automatically print out on the Patient Summary (discharge instructions)
- Patients MUST call to schedule their own outpatient study. Patient should then call TFU afterwards to get the results of the study
- Outpatient CTs, ultrasounds and MRIs are generally booked 4-6 weeks out. PLEASE do NOT tell the patient to schedule the appointment within a few days
- If you think the patient needs the outpatient radiology appointment sooner, you will need to get overbook approval from Radiology during business hours and type the name of the approving Radiologist in the future order radiology request in Cerner. Obviously this is going to be harder to do overnight or on weekend shifts.
- Cerner orders:
- Echocardiogram = CV Transthoracic Echocardiogram
- Exercise Stress Test = CV Treadmill Stress Test or CV Exercise ECG Stress Test
- Holter monitor = CV Holter Monitor
- Barium Enema = RF Barium Enema
- Upper GI = RF Upper GI
- Mammogram = MG Mammogram Digital Diagnostic (indicate left, right or bilateral)
- Breast ultrasound = US Breast
- EMG = EMG 1 Extremity Request
- EEG = EEG
Next Day Clinic NDC Appointments
- Scheduled appointments in Urgent Care Clinic (UCC) within 24-72 hours after an ED visit to avoid inpatient admission for complex medical patients.
- Appointments are Monday through Friday only.
- This is ONLY for DHS empaneled or responsible patients. This is NOT for OOP patients. Refer OOP patients back to their health plan or if required, transfer patient with approval from their health plan.
- Ensure patient requires an URGENT follow-up appointment with an internal medicine provider in UCC. These appointments should be used to avoid an inpatient admission or observation. Other follow up pathways still exist including CCC and with the patient's DHS PCP.
- Ensure patient has transportation to the NCD follow up appointment.
- Ensure we have the correct working phone number of the patient.
- ED clerks are responsible for scheduling the NDC appointments. Appointments should be within 24-72 hours after ED discharge. Once scheduled, the appointment will show up on the ED Patient Discharge Instructions (Patient Summary)under Future Appointments.
- Ensure ED Note is completed before the NDC appointment.
- Patient should be instructed to follow up in Urgent Care Clinic on the date/time of the appointment. ED Clerk will give patient handout with date/time and instructions to go to Urgent Care Clinic.
*If there are no appointments in the next 24-72 hours for APPROPRIATE patients, please page Paul Salama, Director of NDC; Amion...OV IM....Medicine Subspecialty Consults.....Next Day Clinic; Ok to page 24/7.
Appropriate Diagnoses for NDC
- SEE BELOW FOR ADDITIONAL SPECIFIC INFO BY DIAGNOSIS
- CHF exacerbations - without hypoxia, or need for IV drips; give IV diuretic in ED and have patient followup in 24 hrs; NDC can further titrate meds and arrange for ECHO if needed
- Diabetic foot infection/osteo - without sepsis or necrotizing infection; discussed with podiatry and start antibiotics; NDC can re-consult podiatry and obtain further testing as needed
- AKI without signs of shock or underlying electrolyte abnormalities; discuss with renal, consider trial of IVF in ED; NDC can repeat labs in 1-2 days and re-consult renal.
- ESBL infection, known or suspected, without sepsis (e.g. well appearing UTI); give one dose Ertapenem or Amikacin in the ED and have pt return in approximately 24 hrs for culture results and further dosing needed.
- Cellulitis without sepsis that may have failed conventional oral antibiotics; start Linezolid and have patient return in 1-2 days in NDC for a recheck.
- Urgent GI endoscopy for stable patients (must contact GI prior to scheduling NDC appt)
- Cancer, new diagnosis or suspected, or other serious diagnosis/issue requiring urgent follow-up; obtain appropriate imaging in the ED and scheduled for NDC appointment for possible biopsy, and further imaging and testing as needed
- Any other condition that might otherwise be admitted but is suitable for urgent internal medicine follow-up.
NEW July 19, 2024 = CCC now has dedicated slots for new cancer workups. See WikEM...OVMC...CCC
NDC EXCLUSION CRITERIA FOR ALL CONDITIONS
- Lives over 30 minutes away from OV
- Extremely poor social conditions/support based on subjective evaluation
- Must have accessibility to telephone and ability to be contacted reliably
- Not DHS eligible/responsible (must be DHS eligible to be seen in NDC); NO OOP!!!
- Any allograft or autologous stem cell transplant recipient
- Immunocompromised
- Primary condition (e.g., HIV with CD4 count <100, neutropenia with ANC<500, active chemotherapy, not that diabetes does not count)
- Iatrogenic (e.g., ≥20mg prednisone equivalents per day x 3 weeks, chemotherapy, biologics)
- Pregnant
- Resides in SNF/ALF
- History of frequent AMA or no-shows to clinics
- ASA IV classification: “severe systemic disease that is a constant threat to life”
Need Help? For Assistance or Guidance for NDC, call the following:
- NDC Director on-call: Listed on AMION....OV IM passcode
- Hospitalist on duty: place Consult to Hospital Medicine in Cerner
- ED Interim Chief Scott Lundberg: cell number posted in ED
Additional Specific Information by Diagnosis for NDC Appointments
AKI Acute Kidney Injury
- Inclusion criteria for next day clinic:
- Stage 1 AKI (Cr 1.5-1.9 times baseline) or stage 2 AKI (Cr 2.0-2.9 times baseline)
- If there is suspicion for UTI/pyelo, refer to that algorithm instead
- Illness-specific EXCLUSION criteria for next day clinic (in addition to general exclusion criteria):
- Toxic ingestion
- New or worsening oliguria (<0.3cc/kg/hr x 24 hours)
- Anuric for >12 hours
- Patient presents with clinically significant hypervolemia
- Decompensated cirrhosis
- New or worsening oxygen requirement
- Any of the following laboratory abnormalities: pH<7.30 (if applicable), K>6.0, BUN>50
- UA: Gross hematuria, microscopic hematuria with >5 RBCs/HPF, cellular casts
- New proteinuria >300 mg/dL (worsening proteinuria is acceptable)
- Stage 3 AKI (Cr more than 3.0 times baseline), or if Cr >3.0 with unknown baseline
- New hydronephrosis on imaging
- High suspicion for obstructive stone that may require intervention
- Post-obstructive AKI with PVR greater than 250cc
- Treatment in ED
- If any exclusion criteria present on H&P then stop algorithm and deliver care as usual.
- If BMP reveals bicarb <18, then draw VBG.
- If pH < 7.30 then stop algorithm and deliver care as usual.
- If patient has diabetes or there is concern for BPH/obstructive picture, ensure PVR is obtained in ED.
- If PVR >250cc, the stop algorithm and deliver care as usual.
- Ensure a STAT renal ultrasound is obtained in ED unless clear pre-renal picture (e.g. vomiting/diarrhea).
- If new hydronephrosis, then stop algorithm and deliver care as usual.
- Administer 1 to 3 liters of IV crystalloid based on clinical judgment (ideally over 1.5L if safe).
- Schedule for NDC appt for the following day (approx 24hrs)
NDC Cellulitis (excluding diabetic foot infections)
- Inclusion criteria for next day clinic:
- Cellulitis that would typically be admitted (i.e., not usual candidate for oral cephalosporin)
- Cellulitis that “failed” oral cephalosporins as outpatient are great candidates
- Illness-specific EXCLUSION criteria for next day clinic (in addition to general exclusion criteria):
- Diabetic foot infection-- refer to that algorithm instead
- Necrotizing skin/soft tissue infection
- Evidence of sepsis
- Treatment with IV antibiotics of the same site within the prior month
- Cellulitis of the face, hands, or overlying joints
- History of limb amputation or complex skin/soft tissue infections in the past
- Severe penicillin allergy (e.g., SJS/TENS), non-severe PCN allergy is okay
- Treatment in ED:
- Use sharpie to outline borders of affected area, and follow the appropriate pathway below
- For Pus/Purulent Infections
- 1. Ensure I&D is performed in ED and sent for culture, and give one of the following antibiotics:
- For standard patients who can be discharged on oral cephalosporins, they do not need NDC follow-up
- For patients who would normally be admitted, give 600mg Linezolid PO/IV
- Discharge with Linezolid 600mg PO BID x7 days
- If contraindication to Linezolid (e.g., SSRI/TCA), give Vancomycin 1g IV (may require renal dosing)unless already given.
- Discharge with Minocycline 200mg po loading then 100mg BID x7 days (MRSA resistance <10%)
- Alternatively can use 7d Bactrim 2 DS BID or Doxy 100mg BID, but MRSA resistance >10%
- If concern for compliance, follow-up, drug use, etc., on-call pharmacist can approve 1.2g Oritavancin IV
- Please use sparingly. Does not require outpatient antibiotics after Oritavancin.
- 2. Proceed to Schedule Follow-up
- 1. Ensure I&D is performed in ED and sent for culture, and give one of the following antibiotics:
- For Animal/Human Bite Infections
- 1. Assuming patient has received Ampicillin-Sulbactam, schedule another 3g dose 4-6 hours after last
- Discharge with Amoxicillin-Clavulanate 500mg q8h x7 days
- 1. Proceed to Schedule Follow-up
- 1. Assuming patient has received Ampicillin-Sulbactam, schedule another 3g dose 4-6 hours after last
- For Non-Purulent Standard Cellulitis
- 1. For standard patients, give 600mg Linezolid PO/IV (if no contraindications)
- Discharge with Linezolid 600mg PO BID x7 days
- If contraindication to Linezolid (e.g., SSRI/TCA), pursue Oritavancin with on-call pharmacist
- If concern for compliance, follow-up, drug use, etc., on-call pharmacist can approve 1.2g Oritavancin IV
- Please use sparingly. Does not require outpatient antibiotics after Oritavancin
- 2. Proceed to Schedule Follow-up
- 1. For standard patients, give 600mg Linezolid PO/IV (if no contraindications)
- Schedule Follow-up
- 1. Schedule Next Day Clinic in-person appointment within 24 hours for another dose of IV antibiotics (Linezolid, Vancomycin, Ampicillin-Sulbactam, or Ceftriaxone)
- Schedule NDC in-person appointment in 24 hours, instruct patient to hold oral antibiotics 12 hours prior
- 1. Schedule Next Day Clinic in-person appointment within 24 hours for another dose of IV antibiotics (Linezolid, Vancomycin, Ampicillin-Sulbactam, or Ceftriaxone)
NDC Diabetic Foot Ulcer and/or Osteomyelitis
- Inclusion criteria for next day clinic:
- Diabetic foot ulcer with or without concern for osteomyelitis
- Lower extremity osteomyelitis with or without overlying skin infection
- Any cellulitis in a patient with diabetes that does not meet the exclusion criteria
- Illness-specific EXCLUSION criteria for next day clinic (in addition to general exclusion criteria):
- Concern that patient will require surgical intervention beyond simple bedside debridement
- Necrotizing skin/soft tissue infection or wet gangrene
- Unstable vitals
- Evidence of sepsis
- Treatment with IV antibiotics of the same site within the prior month
- Severe penicillin allergy (e.g., SJS/TENS); non-severe PCN allergy is okay
- Treatment in ED:
- 1. Use sharpie to outline borders of affected area
- 2. If wound probes to bone OR xray/CT suspicious for osteomyelitis:
- a. Consult to podiatry for debridement/deep wound culture/bone culture in ED
- b. If podiatry consult unavailable in ED can organize podiatry follow-up from the NDC
- c. MRI to evaluate for acute/chronic osteomyelitis can be completed in NDC
- 3. If wound does not probe to bone:
- a. Obtain standard wound cultures
- 4. If evidence of surrounding necrotic tissue, consult podiatry for ED debridement
- a. If podiatry unavailable in ED and urgent debridement is necessary, can admit
- b. Otherwise, non-urgent podiatry debridement can be organized in NDC
- 5. If there is no current skin/soft tissue infection, then give no antibiotics (cultures will be followed)
- a. Proceed to Schedule Follow-up
- 6. If there is concurrent skin/soft tissue infection:
- a. Give Ampicillin/Sulbactam 3g IV x1 regardless of if there is purulence
- ● Discharge with Amox/Clav 875mg pO q12h x7d (dosing must be adjusted for renal impairment unless otherwise specified)
- ● If h/o MRSA, give Minocycline 200mg PO x1 (loading), then discharge with 100mg PO q12h x7d
- MRSA has much lower resistance rates to mino than doxy/bactrim, but these can be used as alternatives
- a. Give Ampicillin/Sulbactam 3g IV x1 regardless of if there is purulence
- 7. Proceed to Schedule Follow-up
- Schedule Follow-up
- 1. If further IV antibiotics needed for cellulitis: Schedule Next Day Clinic in-person appointment within 24 hours
- Schedule NDC in-person appointment in 24 hours; instruct patient to hold PO antibiotics 12 hours prior.
- 2. If no further parenteral antibiotics are necessary and no deep wound/bone cultures are needed.
- Schedule NDC appointment in 1-5 days. Follow-up interval based on severity of infection using clinical judgment. If non-severe, schedule follow-up after cultures expected to result.
- 1. If further IV antibiotics needed for cellulitis: Schedule Next Day Clinic in-person appointment within 24 hours
NDC Gastrointestinal (GI)Urgent Cases
- Gastrointestinal bleeding or suspected bleeding
- Dysphagia or odynophagia
- Clearly abnormal imaging studies suggestive of malignancy
- Significant, unintentional weight loss not explained by other causes, warranting bidirectional (endoscopy and colonoscopy) in expedited fashion
- INCLUSION criteria
- 1. No vomiting of bright red blood witnessed during ED stay
- 2. Hemodynamically stable
- 3. Hemoglobin stable when compared to baseline or near normal limits
- 4. Patient must not be taking warfarin, NOAC's, or enoxaparin (Lovenox)
- 5. INR level must be <1.5 and platelets >50
- 6. Patients must be tolerating at least liquids; any patient unable to take POs should be admitted
- 7. Patients with evidence of luminal GI obstruction, impending obstruction or food impaction/foreign body obstruction should always be admitted
- Management in the ED
- 1. Discuss case with on-all GI fellow or attending who will decide if patient is appropriate for NDC follow-up appointment. DO NOT SCHEDULE NDC APPT FOR GI WITHOU DISCUSSING WITH ON-CALL GI FELLOW OR ATTENDING.
- GI fellow or attending may be able to schedule an outpatient procedure without a NDC appt; NDC appts are for patients who would otherwise be admitted
- Please confirm with GI fellow or attending that an NDC appt is necessary to expedite the procedure prior to scheduling the NDC appt
- When clerk schedules the NDC appt, please have ED clerk write "endoscopy evaluation" in the field that queries reason for visit
- GI can accommodate Tuesday - Friday AM appointments; NOT Monday AM appts
- Patient will likely be evaluated by both GI and anesthesiology during the NDC appt; patient will then be given another appt and instructions to return directly to OPSA for the procedure(s).
- 1. Discuss case with on-all GI fellow or attending who will decide if patient is appropriate for NDC follow-up appointment. DO NOT SCHEDULE NDC APPT FOR GI WITHOU DISCUSSING WITH ON-CALL GI FELLOW OR ATTENDING.
NDC Pyelonephritis or Acute Cystitis
- Inclusion criteria for next day clinic:
- Any uncomplicated or complicated UTI (including pyelonephritis) that does not meet the exclusion criteria
- History of MDR organisms (including ESBL) are acceptable
- Frequently recurrent UTIs are acceptable
- Illness-specific EXCLUSION criteria for next day clinic (in addition to general exclusion criteria):
- New or worsening oliguria (<0.3cc/kg/hr x 24 hours)
- Anuric for >12 hours
- Patient has unstable vitals and/or high suspicion for bacteremia
- Stage 3 AKI (Cr more than 3.0 times baseline)
- Evidence of stones that are a suspected nidus of infection
- Treatment in ED for all Pyelonephritis and Cystitis (including history of ESBL)
- 1. For standard cases without complex antimicrobial history, deliver care as usual (e.g., ceftriaxone 1g)
- 2. If ESBL or CRE organisms within prior 12 months, administer amikacin 15 mg/kg IV (renal dosing)
- a. Can also give if high suspicion for ESBL: recent (within 2-3 months) antibiotic use or prolonged hospitalization, presence of foley, resides in nursing home
- 3. If Cr>1.5 and concern for ESBL, prescribe 1g Ertapenem IV
- a. Please only use carbapenems in renal impairment given risk of c.diff and PRIME penalties
- 4. For pyelonephritis, discharge with one of the following enteral antibiotics:
- a. No h/o ESBL: Cefdinir 300mg BID x 14 days (renal dosing)
- b. H/o Zosyn-sensitive ESBL: Augmentin 875mg BID + cefdinir 300mg BID x 14 days (renal dosing)
- i. In addition to POs, 100% of these patients will return to NDC for Amikacin/Ertapenem
- c. H/o fluoroquinolone-sensitive isolates: Ciprofloxacin 500mg BID x 7 days (renal dosing)
- d. Other difficult susceptibility profiles can be addressed in NDC-- discharge with plans for IV abx
- 5. For acute cystitis, discharge with one of the following enteral antibiotics:
- a. If creatinine clearance > 60: Nitrofurantoin 100mg BID x 7 days
- b. If creatinine clearance < 60: Fosfomycin 3g x 1 dose
- c. If h/o enterococcus: Amoxicillin 500mg PO q6h x7 days (if PCN allergy: Nitrofurantoin 100mg BID)
- d. Other difficult susceptibility profiles can be addressed in NDC-- discharge with plans for IV abx
- 6. Proceed to Schedule Follow-up
- Schedule Follow-up
- 1. If patient presented to the ED with a foley catheter or suprapubic tube in place, replace the catheter
- 2. If clinical judgment suggests additional dose of parenteral antibiotics is necessary (either Amikacin 15mg/kg, Ceftriaxone 1g q24h, or Ertapenem 1g q24h for h/o ESBL)
- 3. Schedule Next Day Clinic in-person appointment within 24 hours
OOP (Out of Plan)
- Orange OOP on Tracking Board indicates out of plan insurance. Patient should be referred back to their health plan and PCP.
- Info on health plan and PCP found on Patient Summary (Discharge Instructions), Demographics and Utilization Review tabs.
- Do not refer OOP patients to subspecialty care at OVMC
- OOP Health Plan and/or clinic name will print automatically on the Patient Summary (Discharge Instructions).
- URGENT FOLLOWUP: To arrange urgent followup with PCP for OOP patients, call Outpatient Service Coordinator (OPSC) x74556. After hours/weekends/holidays, leave message with patient name, MRUN, and reason for urgent followup (e.g. fracture, new lung mass, etc). Make sure contact info is correct in Cerner. OPSC coordinators will help expedite a followup appt with the PCP. Remember,outside health plans usually require patients to see their PCP before being referred to a subspecialist.
DHS Empaneled
- To find out if a patient is empaneled to a DHS provider, look at the banner bar on the patient's chart. Look right hand side "Emp Prov". Name of PCP will be written there.
- If empaneled, DHS or community clinic name can be found listed under Additional Patient Information on ED Summary page.
- URGENT FOLLOWUP: To arrange urgent followup with PCP for OOP patients, call Outpatient Service Coordinator (OPSC) x74556. After hours/weekends/holidays, leave message with patient name, MRUN, and reason for urgent followup (e.g. fracture, new lung mass, etc). Make sure contact info is correct in Cerner. OPSC coordinators will help expedite a followup appt with the PCP. Remember,outside health plans usually require patients to see their PCP before being referred to a subspecialist.
MHLA (My Health LA)
- Indicated by green MHLA icon on tracking board
- Not an insurance plan but gives patient access to primary care clinic and provider (PCP)
- MHLA patients receive all SPECIALTY care at OVMC or other DHS facilities
- OK to refer MHLA patients to subspecialty care at OVMC either through Message Pool or econsult.
NERF (New Empanelment Referral Form)
- Used to enroll patients with significant PMH who have no primary care or health plan
- Patient must have at least one of a specific list of diagnoses
- Only about 1/3 of patients will actually receive a PCP through the NERF process. Because of that, give patient a clinic list upon discharge so he/she can find a PMD on their own.
- To enroll in NERF program, click NERF while completing Depart process. Check off diagnoses that apply. Click green arrow. Clerk will complete on-line NERF form. OR. Open patient's chart. Go to Primary Care Information at the bottom of the tabs on the left. Click New Empanelment. Complete form. Unless patient has strong desire to be empaneled to a particular primary care clinic, leave options open.
TFU (Telephone Follow Up)
- 818-364-4825 (STAFFED ONLY 2 DAYS PER WEEK!!!) DO NOT USE TFU FOR ANYTHING URGENT or EMERGENT!!!
- Used for follow-up of culture or GC/chlamydia results and for patients to call for outpatient Radiology imaging results
- To refer to TFU, click ED Post Visit Plan while completing Depart process, choose ED-TFU-OVM and indicate what needs to be followed up
- Ensure we have a correct phone number on the patient
- If patient has already been discharged from the ED and you want to refer to TFU
- Step 1: Find patient on the Look Up track (only good for 7 days after discharge)
- Step 2: Choose patient on the Look Up track, click Modify Events.....Request Event......Post Visit ED TFU
- Step 3: Open patient's chart......Depart.....now fill out ED Post Visit Plan form
- If you do not follow these steps, TFU will not be flagged to follow-up the patient
CCC (Continuing Care Clinic)
- ED Followup Clinic used for complicated patients without primary care or an outside health plan
- Guidelines for CCC: Urgent follow-up of potentially serious internal medicine conditions that might otherwise require hospital admission, ED return visits, or extensive ED workup. The clinic is for patients without any other primary care resource; patients who have insurance and/or an established primary care clinic should be referred back there for follow-up of such conditions. *Consults sent to CCC will be reviewed within a few days by the NP who staffs the clinic; patients who have insurance or who do not meet the referral criteria listed below will not be seen in CCC; they will be referred on for routine primary care.
- Our DEM TFU program can also refer patients to CCC, so if a test is pending to determine whether a patient meets criteria, please do not generate a CCC referral; the TFU program can review the test and refer to CCC if appropriate.
- The CCC clinic can coordinate work-ups for possible malignancies including ordering additional outpatient imaging and biopsies.
- Step 1: Please do not skip this step! Ensure that patient does not have established HMO insurance, other primary care. Do NOT send DHS Empaneled or OOP patients (see DHS Empaneled and OOP).
- Step 2: Click ED Post Visit Plan while completing Depart process, choose ED-CCC-OVM
- Step 3: Indicate condition requiring urgent CCC visit:
- Suspected new or recurrent neoplastic disease: NEW July 19, 2024 - new dedicated CCC slots on Fridays for new cancer workups; goal to decrease admissions for cancer workups. Patient must be hemodynamically/metabolically stable (ie no concern for tumor lysis syndrome, blast crisis, etc). Solid tumors and very stable potential lymphomas are the best patients. If there is concern for visceral crisis, then please consult Heme/Onc first, but otherwise not necessary to do so in order to place referral. Please indicate "Expedited Malignancy Workup" as the reason for the CCC referral.
- Acute medical condition potentially requiring inpatient admission if not followed up promptly
- Diabetes out of control (Glucose >500, requiring initiation of insulin therapy, or new end-organ dz.)
- Severe hypertension (>160/100 at time of ED discharge, new end-organ dz., or refractory to tx.)
- Suspected new significant auto-immune disease (SLE, RA, scleroderma, IBD, vasculitis)
- Complex or undefined infections requiring further evaluation (FUO, osteo, colitis, fungal/parasite, HIV)
- Acute pulmonary disease or exacerbation requiring systemic steroids or antibiotics
- Potentially serious lab or imaging findings (anemia, hepatitis, renal insuff., hyperCa++, incidentalomas)
- Endocrine disease requiring advanced workup (hyperthyroidism, thyroid masses, pituitary/adrenal dz)
- New congestive heart failure, arrhythmia, or structural cardiac disease not requiring admission
- Decompensated liver disease requiring diuretics, paracentesis, or workup for occult etiology
- New or recurrent deep venous thrombosis or other condition requiring anticoagulation
- If you have questions about a consult, or wish to discuss a case during regular business hours, contact Dennis Chamling, NP, via the Department of Medicine or by pager on the amion.com internal medicine website. (password ov_im)
Urgent Referrals for Subspecialty Care/Message Pools
- Used to refer patients to certain subspecialty clinics for URGENT follow-up appts (<4 weeks)
- Do NOT refer OOP patients or non-urgent complaints through the Message Pool
- For Colorectal, ENT and Ophtho patients, page the on-call resident for approval for the urgent follow-up appt. Type in the approving resident's name and the follow-up date/time agreed upon. Tell patient to show up at 8am to the clinic.
- Current Clinics with Message Pools:
- OVM Colorectal ED/UC Urgent Follow up - needs 24/7 phone call to general surgery
- OVM Coumadin ED/UC Urgent Follow Up
- OVM Hand Surgery ED/UC Urgent Follow Up
- OVM Gyn Aftercare ED/UC Urgent Follow Up
- OVM Interventional Radiology ED/UC Urgent Follow Up
- OVM MAT Bridge ED/UC Urgent Follow Up
- OVM Ophthalmology ED/UC Urgent Follow Up - needs 24/7 phone call to ophtho
- OVM Orthopedics ED/UC Urgent Follow Up
- OVM Otolaryngology (ENT) ED/UC Urgent Follow Up - needs 24/7 phone call to ENT
- OVM PCC (HIV) ED/UC Urgent Follow Up
- OVM Pediatrics ED/UC Urgent Follow Up
- OVM Peds Ortho ED/UC Urgent Follow Up
- OVM Plastic Surgery ED/UC Urgent Follow Up
- OVM Podiatry ED/UC Urgent Follow Up
- OVM Procedure Service ED/UC Urgent Follow Up
- OVM Urology ED/UC Urgent Follow Up
- OVM - Trauma Recovery ED/UC Urgent Follow Up
Econsult
- eConsult appointment center for new referrals: 747-210-3800
- eConsult is now accessed directly through Cerner from within a patient's chart. There is an eConsult tab available under the Table of Contents Menu (Table of Contents are the grey tabs on the left hand side of the mPage underneath the "ED Summary"). Users no longer have to manually enter patient identifiers to search for a patient. There is no longer a need to maintain a separate username and password for eConsult.
- Used to refer patients to subspecialty clinics for NON-URGENT follow-up appts. Not all referrals are approved. In fact, most from the ED are denied. If approved, appts are likely several months away.
- Do NOT send eConsults on OOP patients
- Do NOT send eConsults on DHS empaneled patients. These patients should be referred back to their primary care doctor.
- For outside records to be attached, use the Fax-to-Scan form on the Econsult. Print it out. Patient name and MRUN will be on the fax form. Attach it to the outside records and give to the clerk to fax. See job aid. XXXXX
- For General Surgery gallbladders and hernia referrals, fill out the Cholecystectomy/Hernia form. Patient must be non-smoker with BMI <35
- Do NOT refer the following:
- Derm - simple skin conditions (must be SEVERE or worrisome for cancer)
- GI - diverticulitis, undiagnosed abdominal pain, gastritis without minimum of 3 months of PPI or h.pylori treatment
- Neuro - simple seizures, headaches
- Urology - stones less than 5mm
Patient Education
Diabetic Teaching
- Classes held at OVMC; patients must call to schedule a class, 747-210-3176
- Classes are 9am-12:30pm
- Appointment is required to attend class; late arrivals will not be allowed to participate
- Adult Classes English http://myladhs.lacounty.gov/ov/Departments/Education/Documents/CommunityClasses/Diabetes%20Self%20Management%20Group%20Education%20Flyer_English.pdf
- Adult Classes Spanish http://myladhs.lacounty.gov/ov/Departments/Education/Documents/CommunityClasses/Diabetes%20Self%20Management%20Group%20Education%20Flyer_Spanish.pdf
Cardiology
Code STEMI
- Definite STEMI on EKG and appropriate patient - ACTIVATE Cath Lab per protocol below
- Probable STEMI or complex patient - CONSULT Cardiology (digital FAX 310-496-0160)
| Oliveview UCLA Medical Center | Providence Holy Cross |
| Mon-Fri 7am-5pm | Nights, weekends, holidays |
| Page Code STEMI via Cerner Consults- Auto Paging (pager 818-226-4502) | Verbally concept patient for transfer |
| Verbally consent patient and family for PCI | Fax the EKG to Holy Cross: 818-496-4495 |
| Goal: <30 mins in ED | Call 818-496-7700 (or 7704) for Patient Placement Center to start the Code STEMI transfer |
| ***Speak with ED physician at Holy Cross to review the faxed EKG | |
| ***Chart accepting MD name | |
| For updates, call ED direct 818-496-1270 | |
| Call LAFD 213-847-5340 (or 5360) for Code STEMI transfer | |
| ***Emergency STEMI transfers ONLY | |
| ED Clerk to fax patient registration info to 818-496-7707 | |
| Goal: <45 mins in ED before transfer |
- DEFIBRILLATOR DEVICE AT PATIENT BEDSIDE FOR ALL STEMI's
- ED: Zoll pads package at bedside (apply only if unstable)
- OVMC Cath Lab: Cardiology will bring & apply radiolucent Zoll Pads
- Transfers: LAFD uses Physio monitor. Pads applied PRN arrhythmia.
| Primary Medications | Optional Medications | Nursing Duties |
| Aspirin 325mg P.O. | Nitroglycerin (SL or patch) | Undress patient |
| Heparin 5,000 U bolus IV | Morphine IV | Two saline locks |
| Defer 2nd anti-platelet drug to cardiology's choice | Ativan IV | Hang one bag saline, slow drip |
| AVOID intravenous drips | At OVMC, ED nurse goes with patient to Cath Lab and brings Code Blue kit | |
| For transfers to Holy Cross: call report to 818-496-1270 |
- Plan B Transfer to Northridge
- Rare event of Holy Cross closure or 2 simultaneous STEMI, fax EKG to 818-885-3590 and then call Northridge ED charge nurse at 818-885-5396
Dental
Dental Clinics
- No services available at OVMC
- Dental Clinics https://sslvpn.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/,DanaInfo=myladhs.lacounty.gov+Dental%20Clinics.pdf
- Dental Clinic Mid-Valley https://sslvpn.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/,DanaInfo=myladhs.lacounty.gov+Dental%20Mid-Valley.pdf
Dermatology
Dermatology Clinic Referral Guidelines
- ONLY refer patients through econsult with SEVERE skin disorder or concern for skin cancer
- Referral through econsult MUST include photos
- Clerk has digital camera and USB cable. Camera icon may take a minute or so to show up on "Computer"
- Please delete any photos from camera or desktop after use
Employee Health - Staff Exposure / Needlestick Cases
- Who handles staff exposure cases?
- Business hours - refer patient to Employee Health, closes 4:30pm
- When Employee Health is closed, if UCC is open, send to UCC
- When Employee Health and UCC are closed, staff member to be seen in ED
- Reason patient is seen in the ED at time of exposure is to determine if exposure has high enough risk to warrant presumptive treatment with PEP
- Business hours - refer patient to Employee Health, closes 4:30pm
- Basic Protocol
- No paperwork required; all documentation will be done in Cerner
- Staff member to registered in Cerner; PAC will use IA billing code to register employee
- ED or UCC provider will use .edexposure autotext for documentation of exposure episode
- NO LABS WILL BE DRAWN ON THE STAFF MEMBER FROM THE EMERGENCY DEPARTMENT; ALL lab testing on staff member will occur in Employee Health (or at UCLA for students/residents/fellows) the next business day even over a long weekend and even if PEP meds are started
- Source patient will have labs drawn by unit/clinic using the Blood and Body Fluid - Source Patient order set
- Decision to treat with post-exposure prophylaxis medication
- For any questions regarding the starting of PEP, Consult Infectious Disease 24/7
- If PEP is deemed appropriate, ED provider will prescribe the following medications through Cerner (PRINT OUT HARD COPY OF PRESCRIPTION. DO NOT EPRESCRIBE TO OUR PHARMACY. OK TO PRINT ON WHITE PAPER. GIVE HARD COPY TO ED PHARMACIST WHO WILL GO GET THE MEDICATION):
- Truvada 200/200mg tabs one tab QDAY x 30 days
- Raltegravir 400mg tabs one tab BID x 30 days
- Where do we send for follow-up?
- OVMC employees should be instructed to followup at Employee Health the next business day; just walk-in. No need for appointment.
- For OVMC employees: *Message through Cerner: Suzanna Mendez-Nasrallah NP that employee was seen in the ED for an exposure.
- For UCLA students: Refer back to UCLA Student Health.
- For UCLA resident/fellows: Refer back to UCLA Occupational Health.
- No additional paperwork besides ED Discharge Instructions is given to staff member. All workman's comp paperwork will be completed by Employee Health or UCLA.
- OVMC employees should be instructed to followup at Employee Health the next business day; just walk-in. No need for appointment.
ENT/Head and Neck
Hearing Aids
- Econsult to Audiology who will screen patient with audiology testing and refer to ENT if necessary
Gastroenterology
H. Pylori Testing
- OVMC has removed the H.pylori BLOOD test; all H.pylori testing should be STOOL Antigen testing
GI Clinic Referral Guidelines
- Abdominal pain – do not refer chronic abdominal pain of unclear etiology to GI
- Abnormal imaging
- If radiology reading is clearly suspicious for malignancy, refer to GI
- Do not refer patients with studies that “cannot rule out”, “includes possibility of”, etc.
- Do not refer patients simply because radiology wrote “endoscopy is recommended” on final read. Send patient to PMD or CCC for further interpretation of study results or further imaging
- Anemia - Refer ONLY iron deficiency anemia; send Fe, TIBC, Ferritin; refer to TFU who will place e-consult if labs show iron deficiency
- Barrett’s Esophagus – refer only if documented pathology report can be attached to e-consult
- BRBPR
- If patient is anemic, refer to GI
- If patient is > 40yo, refer to GI
- If patient is < 40yo, Anusol-HC supp qhs x 14 days. Symptoms persist? Follow-up PMD or have pt call TFU for GI referral
- Do not refer if bloody diarrhea
- Cirrhosis – Refer ONLY for banding of esophageal varices
- Constipation – treat with osmotic laxative (e.g. sorbitol/miralax/prune juice) and send TSH if applicable
- If severe (<1 BM per week) or rapid onset, refer to GI
- Diarrhea
- Will only see chronic non-infectious diarrhea >8 weeks; send C&S, O&P, C.diff, WBC; refer to TFU who will place e-consult if stool studies negative
- Diverticulitis – do NOT refer to GI; Pt must be asymptomatic for 2 months before GI will consider colonoscopy
- Dysphagia
- If problem is high in throat region, refer to ENT instead If patient does not have weight loss, send barium swallow
- If patient has weight loss or severe dysphagia, refer to GI
- Dyspepsia (i.e. upper GI pain/epig pain >3 months)
- If patient is > 55yo OR has worrisome symptoms, e.g., weight loss, refer to GI
- If patient is < 55yo, order H. pylori test; refer to TFU who will treat with antibiotics if positive
- If H.pylori test is negative or antibiotic trial fails, try PPI BID for at least 2 months. If that fails, refer to GI for evaluation
- Family history of colon cancer (must be first-degree relative – mom,dad, sister, brother, child)
- If only one relative, must be < 60 at age of diagnosis or if two or more relatives, age of diagnosis is not important
- If patient fulfills above criteria and is either older than 40 or 10 years younger than the age of the relative at diagnosis (whichever is earlier), refer to GI
- Otherwise, refer to primary care for fecal occult blood testing.
- GERD (e.g. burning epig/chest pain with acid taste)
- Do NOT refer to GI – pt must be on maximal therapy x 2months AND have lifestyle changes
- If patient is not on maximum PPI therapy, change to or increase PPI to BID. Ex: Omeprazole 20 mg BID.
- Hepatitis C - Do NOT refer to GI – treatment reserved for compensated cirrhotics; send to primary care
- Inflammatory Bowel Disease
- If urgent referral needed (moderate flare symptoms), call GI Fellow/Attending on-call; otherwise refer to PMD
- Irritable Bowel Syndrome
- Only if associated with worrisome symptoms (sudden onset at late age, weight loss), refer to GI
- Occult positive stool only – do not refer from the ED
- Pt must be >50yo, <50 BMI, AND have CLIA-approved lab occult-positive test NOT from ED to be referred
- Polyps – Do NOT refer to GI unless you can attach endoscopy and pathology reports Ulcer – refer only GASTRIC ulcers that are >5mm; do NOT refer duodenal ulcers
- If concern for malignancy based on outside endocscopy results, call GI for Urgent Consult
- Urgent Consults
- Communicate with on-call GI Fellow/Attending AND place e-consult; Note fellow on call CANNOT overbook a clinic visit
Infectious Disease
Reportable Diseases and How To
- HIV - if HIV diagnosed at OVMC in our lab, then OVMC ID will take care of reporting positive HIV to LA County Health Department. Not emergency to report. ED does not have to report.
- If known HIV patient presents to DHS requesting follow-up, check for OOP then Message Pool OVM PCC(HIV) ED/UC Urgent Follow Up
- PCC = Positive Care Clinic
Dog Bite Reporting Form
http://www.publichealth.lacounty.gov/vet/docs/Forms/BiteFormVet.pdf
Public Health Confidential Morbidity Report Form Reportable Diseases
- Hot Line: (888) 397-3993
- Fax Line: (888) 397-3778 of (213) 482-5508
http://www.publichealth.lacounty.gov/acd/pubs/reports/CMR-H-794.pdf
Public Health STD Confidential Morbidity Report Form
http://www.publichealth.lacounty.gov/dhsp/ReportCase/STD_CMR.pdf
TB Outpatient Management Guidelines
- Revised Oct 2014
- The following symptoms, risk factors, and radiographic findings are associated with active TB disease (adapted from Moran et al, Ann Emerg Med, 2009):
| Symptoms | Risk factors | Radiographic findings |
| Weight loss (>1 month) | History of homelessness | Cavitary lesion(s) |
| Cough (>2 weeks) | History of incarceration | Apical or upper lobe infiltrates |
| Fever (>2 weeks) | Born outside the U.S. | |
| Night sweats (>1 month) | Prior active TB disease | |
| Hemoptysis | HIV infection | |
| Malaise (>1 month) | History of TB exposure | |
| History of (+) tuberculin skin test* | *A positive tuberculin skin test alone does not necessitate collection of sputum for active TB disease |
- EVALUATION OF PATIENTS FOR ACTIVE PULMONARY TB DISEASE IN THE ED
- 1. Perform a History and Physical, asking specifically about the symptoms and risk factors noted in the Table above.
- 2. Order chest radiograph.
- 3. Perform a clinical assessment, taking into account symptoms, risk factors, HIV status, and radiographic findings.
- 4. If active pulmonary TB disease is considered possible, order the following tests:
- 1) AFB Culture, other non-sterile, PHL (sputum induced)
- 2) M. tuberculosis PCR with Rifampin Resistance (sputum or expectorated or induced)
- 3) HIV antigen/antibody screen (blood)
- The first specimen should be collected in the ED and should be induced by inhalation of an aerosol (e.g., warm, sterile, 3%–5% hypertonic saline).
- Further sputum collection (a total of 3 samples q8 hours recommended) can be collected by Public Health (if discharged) or on the ward (if admitted).
- HIV tests will be followed up as an outpatient but will not be performed STAT
- 5. If discharge is appropriate (see criteria below), the patient must be reported to the TB liaison by phone.
- 6. If patient meets all discharge criteria, educate patient and provide written instructions with appropriate infection control precautions (see below).
- DISCHARGE CRITERIA (all must be met)
- Can be discharged to a stable residence with a verified address and phone number
- WILL NOT be discharged to a shelter, nursing home, single room occupancy hotel or other congregate settings
- WILL NOT have significant contact with immunosuppressed individuals or children ≤ 5 yo
- Is willing and able to follow-up with outpatient care
- Is willing and able to comply with home isolation (see below)
- Remember, patient may need a work note
- REPORT TO TB LIAISON
- Call (747)210-4590
- Leave a voicemail with patient name, MRN, patient address AND phone number
- Do not call the County Operator as the message instructs. The Department of Public Health will attempt to locate the patient and ensure they are evaluated further as an outpatient at a public health clinic
- PATIENT EDUCATION - give patient info sheet - located in MD Room or link here https://sslvpn.lacounty.gov/ov/Departments/DEM/Documents/,DanaInfo=myladhs.lacounty.gov+TB%20Patient%20Info%20English.pdf
- DO NOT receive visitors at home, visit others, or go to work until evaluated by Public Health
- DO NOT care for children ≤ 5 years old
- Avoid public areas/ public transportation.
- If you are employed DO NOT go to work
- Cover your mouth and nose when coughing
- Wear a surgical mask when spending time in a shared space (should be provided to patient upon discharge)
- Patients will be contacted regarding any positive TB or HIV results
- FREQUENTLY ASKED QUESTIONS ABOUT TB
- What is the role of the TB liaison at OVMC?
- The primary role of the TB liaison is to assist with patients suspected to have active TB disease, particularly to ensure proper reporting to the Department of Public Health
- Per the new ED policy, the liaison SHOULD be contacted by phone for patients with sputum collected for TB evaluation, but not admitted to the hospital. This is essential to ensure those patients are adequately followed for outpatient evaluation in the public health clinics.
- The liaison SHOULD NOT be contacted for patients with latent TB infection (see below) who are not suspected to active TB disease
- The liaison can also provide information regarding patients seen in the ED who are already diagnosed with TB disease, and may be presenting with a related complaint (e.g., intolerance of anti-TB medications)
- Then liaison is not able to provide clinical consults regarding patient care or decisions to admit/discharge
- How do I contact the TB liaison?
- The liaison has an office at OVMC, and is available Monday through Friday, 9am-5pm.
- Call (747)210-4590; if no one answers, leave a voicemail with the patient’s name and MRUN. VERIFY ADDRESS and PHONE NUMBER ARE CORRECT IN CERNER!
- If calling outside business hours, just leave a voicemail with above information.
- What should I do with a patient sent to the ED for a positive tuberculin skin test (i.e., PPD) or a positive IGRA (e.g., Quantiferon)?
- Both of these tests may represent latent TB infection.
- Patients with a positive test should be evaluated with:
- 1. A history and physical - to see if they have any signs or symptoms or active TB disease.
- 2. A chest radiograph - to look for active pulmonary tuberculosis.
- If the patient’s overall clinical presentation is very unlikely to represent active pulmonary TB (e.g., normal chest x-ray, not immunosuppressed, no signs or symptoms of TB), then the patient should be referred for possible treatment of latent TB infection.
- Preferably, patients should be sent to a primary care provider
- For patients without a primary care provider, they can be sent to public health centers http://publichealth.lacounty.gov/locator.htm
- DO NOT contact the TB liaison for patients with latent TB infection; the liaison should only be contacted for patients suspected to have active TB disease
- What is the role of the TB liaison at OVMC?
MONKEYPOX
ACEP Monkeypox Field Guide: https://www.acep.org/monkeypox-field-guide/cover-page/
=How Transmitted?
- Transmitted via direct contact and respiratory droplet; wear appropriate PPE.
- Place suspects in a room with closed door and 'special precautions' sign
How to Test?
- Use same swab used for COVID testing (UTM or VTM); use one swab to sample 1-3 lesions of the same type, preferably from different locations on the body
- if different appearing lesions, collect additional swabs from several more lesions
- limit 2 swabs per patient
- Order is in Place Orders page (left side scroll down) = Monkeypox Virus DNA Qual RT PCR-SO (if possible, try to unroof the lesion to swab)
- Have low threshold for also testing for HIV
- If you are also swabbing for other things such as HSV, varicella or GC/Chlamydia, make sure you send separate swabs for the other tests
When will results return?
- Tests are send-outs with results taking 3+ days to return
- LA Public Health is notified of all positive results and will follow up with patient for contact tracing and isolation.
DHS also has a centralized process to follow up on positive results and contact patient for consideration of Tecovirimat.
- Consider TFU if you are sending other tests, or if you would like patient notified of negative result
Who to Notify?
- For SUSPECTED cases, contact OVMC Infectious Disease and Prevention x73624; after hours, leave message with patient's name, MRUN, birthdate and verified contact information
What about Treatment?
- Cases treated once confirmed positive; treatment will be handled by OVMC Infectious Disease and Prevention
Discharge Instructions
- Discharge ALL SUSPECTED cases with the LA County Dept of Public Health monkeypox home isolation guidelines
- LA County DPH monkeypox home isolation guidelines now available in Cerner...Patient Education...Departmental...Monkeypox, english and spanish versions available.
- Hard copies of the isolation guidelines also located in ED1A Provider Room
- ED1A clerks have original copies of handouts
How to keep track of staff exposures?
- Nursing will keep track by placing a log sheet outside the patient's room. Names of any staff who enter the room should be added to the log.
What if I have an occupational exposure?
- Monkeypox is not as highly contagious as COVID and many other infections. However, if you come into direct skin contact with any lesions, or are in proximity to an aerosol generating procedure (intubation, swabbing of unroofed lesions) without N-95 mask and face covering then it could be a high risk exposure.
- OV Employee Health has monkeypox vaccine for high risk occupational exposures. You can contact them at x73403
COVID-19
PPE
- All patients should be wearing a mask and presumed contagious even if asymptomatic.
- Visitors should be minimized to one visitor maximum, and only for pediatrics, elderly/disabled in need of assistance, or end of life.
- All staff should wear a mask at all times. Staff who may become involved in aerosolizing procedure may wear an N95 mask throughout shift, at their own discretion. Eye protection should be worn for all patient interactions.
- Patients with fever and/or respiratory symptoms will be moved into an ED room or another care venue after ICN. Those deemed possible COVID suspects will be placed in droplet and contact precautions while in ED.
- Mask, eye protection, gown, and gloves for all COVID-suspect patient interactions. N95 or CAPR/PAPR required if aerosol generation.
- CAPR face shields re-used: clean with purple top wipes; Used N-95 masks in designated white bins to reprocess if not visibly contaminated.
Oxygen Therapy
- Regular nasal cannula or simple/NRB facemask are not aerosol-generating, use first-line (leave paper mask on patient over cannula)
- AVOID CPAP and BiPAP as these are aerosol-generating
- High-flow nasal cannula may be used in with a simple mask over the nose/mouth in patients requiring >10 L/min O2. Limit flow rate to 30 L/min or less. These patients should be placed in airborne isolation.
- Intubation/mechanical ventilation should be considered early enough to allow for careful, planned procedure
Intubation
- N95 with eye protection or CAPR/PAPR. Minimize personnel in room (RN, RT, and 2 MDs). Use negative pressure rooms.
- RSI without bagging whenever possible; If bagging needed, put viral filter (from RT) and place LMA to minimize aerosol generation
- Senior resident or attending to perform. Use Glidescope whenever possible to reduce exposure
- McGrath in the black airway toolbox is only for attending intubation in 2F
- Consider additional protective barrier such as clear sheet if available
- Patients in cardiac arrest: Prioritize intubation over chest compressions if no shockable rhythm.
- Use lung protective vent settings, 6 cc/kg tidal volume with escalating PEEP needed to maintain oxygenation. Simple vent mode (AC)
Treatment of Bronchospasm
- Avoid nebulized therapy as this is aerosol-generating
- In addition to MDI’s, consider sub cut. epinephrine (0.3 mg) or terbutaline (0.25 mg), or IV magnesium
- Steroids should be used as needed; do not withhold based on COVID concerns.
Admission
- Only for persistent oxygen requirement, or some other physiologic derangement (e.g. sepsis). Document PUI for interqual purposes.
- No Observation beds now; Try to dispo with 6-8 hrs (e.g., Asthma, CHF exacerb, CP w neg trops w/o need for risk strat); Otherwise admit.
- Notify hospitalist of COVID suspect. They will coordinate bed choice with ID attending (You do not need to call ID.)
- ANO/patient flow should be contacted for prolonged boarding issues at x73170.
- Consider ICU for patients:
- on ventilator
- requiring >6L/min of oxygen
- requiring pressor support
- with three or more of: AMS, uremia, tachypnea >30, multilobar infiltrate, age >55
- Cover for CAP as appropriate. Other therapy is at discretion of IM/ID/Pulm/ICU teams
- Labs: CBC, CMP, phosphorus, magnesium, LDH, troponin, CK, CRP, ferritin, procalcitonin, PT/PTT, d-dimer.
- Imaging: portable CXR only unless high suspicion of PE or other life-threatening concern besides COVID
COVID and PEDIATRICS
- Any child under age 1 with fever more than 4-5 days (even in the ABSENCE of any Kawasaki’s symptoms/criteria) should be considered a suspect and should be sent for COVID testing, CBC, ESR, and CRP and consider specialty consult with Peds ID/Immune/Cards.
- Any child >1 year of age and up to 18 years of age with fever more than 4-5 days AND any other Kawasaki’s symptom(s)/criteria should be evaluated as above.
COVID Testing Reminders
- Admissions - ordered as Symptomatic or Asymptomatic - all done rapidly (rapidly = a few hours)
- Psychiatric - see below
- Outpatient - Symptomatic, CAN'T Isolate - Do NOT discharge until COVID result is back. Should be used rarely for those living in group homes, SNFs, board&cares. Living with Grandpa doesn't qualify.
- There are hotels/shelters that can be arranged for the rare COVID+ who cannot isolate at home. Can be arranged through social work Mon-Fri business hours. Or patients can be given the DPH number (833) 596-1009 to call themselves.
- Outpatient - Symptomatic, CAN Isolate - These patients should be sent home. Results are sent in a daily report from the lab to our ED COVID RESULTS TEAM. No need to flag anything. Results will be followed up by the team. Including peds cases.
- Make sure we have the correct address and phone number in Cerner.
- Results take 3-5 days. NEGATIVE results will receive a letter in the mail. POSITIVE results will get a phone call.
- Patients can call 747-210-3110, Mon-Fri 8am-4pm, if they have questions. Do NOT refer to TFU.
- Use COVID OVMC Awaiting Testing Results patient handout in the Departmental folder, English and Spanish.
- Asymptomatic or just COVID exposures - Do NOT send tests on these. We do not have the staff to follow these up. Refer to L.A. City website. Coronavirus.lacity.org/testing See new handout in Departmental Folder. COVID OVMC Testing Sites. English and Spanish available.
- Access Center (on the ED Post Visit Plan page) gets the SYMPTOMATIC COVID+ or PUI patient a follow-up phone call with a DHS doctor in about 3 days. This is to find patients who may be getting worse at home. For DHS empaneled or DHS eligible. NOT OOP or MHLA. Check contact phone number in Cerner.
- HOMELESS: For symptomatic patients experiencing homelessness who are going to be placed in a COVID-19 shelter by Social Worker, order as "Outpatient CAN self isolate". These will be held as lower priority as SW will send patient to a shelter where patient will self-isolate while test is pending.
- CONGREGATE LIVING, symptomatic patients: e.g. group home, SNF. Order as "Outpatient CANNOT self-isolate". These will be given priority as discharge may depend upon test results.
- DHS Healthcare Workers: Refer to employee health for testing to x73403. They will get an appt for drive-thru testing 1-3pm weekdays.
Psych Patients and Testing
UPDATED 6-3-2021
- If medically cleared from triage or ambulance bay, and asymptomatic, then no covid testing needed prior to going to psych. If symptomatic, order covid.
- If in an ED bed and medical clearance occurring/waiting for psych to see patient, order the covid test on ALL psych patients. If asymptomatic AND psych has a place to hold the patient awaiting test results, patient can be sent to psych before test results are back. If they don't have a place to hold the patient, then we need to wait until results are back.
Safer at Home/Home O2 and Pulse Oximeter Program UPDATED 12-1-2020
- Candidate for Home O2:
- Should be considered for any suspected COVID-19 patient when:
- Diagnosis of COVID-19 (+) or PUI for COVID-19
- Room air O2 sat < 93% with no history of chronic lung disease
- O2 requirement are 0-3L NC to keep SaO2 >/= 94% or improving clinical trajectory with SaO2 >/= 92%, and without accessory muscle use
- No other medical issues necessitate inpatient care
- Patient has to have access to electrical plug for oxygen concentrator.
- Should be considered for any suspected COVID-19 patient when:
- Step 1: Call Resp Therapy. ED RT x75581 (Supervisor RT x75038 Mon-Fri 8am-8pm-ish); RT will coordinate with oxygen vendor for oxygen and concentrator.
- Patient must remain in ED until oxygen and concentrator arrive from oxygen vendor.
- CalOx Home Health 323-255-5175
- Supercare Health 855-621-5929
- Step 2: ALL STAFF: Verify address and phone number in Cerner
- Step 3: ALL STAFF: Notify ED Clerk to obtain pulse ox ; ED clerk will log patient in the Home O2 binder.
- Step 4: Provider orders DME for Home Oxygen and Home Oximeter Device
- Home Oxygen: Concentrator; continuous flow 1-3 Lpm; interface – nasal cannula; Est need in months – 1; diagnosis – suspected coronavirus.
- Home Oximeter: Pulse ox; hypoxia/coronavirus
- Step 5: Nursing: Have all prescription sent to the ED
- Step 6: RT will educate patient on oxygen cylinders and concentrator when they arrive.
- Step 7: Provider adds COVID discharge instructions
- COVID OVMC Home O2/Safer at Home Discharge Instructions
- COVID OVMC Self-Proning positions Eng/Span
- Step 8: Provider adds Access Center to depart process. This allows patient to have a follow-up call by PCP or CCC within 3 days. OOP patients should be told to call their PCP.
- Step 9: Next Day - ED Clerk assigns NP to call ED patients for 1st follow-up call. Patient will also receive follow-up call 3 days later by PCP or CCC via Access Center. NPs do NOT call Obs or Admitted patients sent home on O2.
- Step 10: NPs document short note after discussion with patient. Message can be left with patient to call ED with questions. No other follow-up calls will be made.
- For any problems, call or text Dr. McCollough 310-614-5306
Discharge Handouts including Department of Public Health
- Prone Positioning https://lacounty.sharepoint.com/:b:/s/dhs-ov-emergencymedicine/ESvTpwAfVz1FllL55FBMVNABobW54lHuSSzUAW83ok2e0A?e=uBf5CV
- Home Care Instructions - Respiratory Symptoms, Not Tested, English
- Home Care Instructions - Respiratory Symptoms, Not Tested, Spanish
- Isolation Instructions - Exposed Household Members, English
- Isolation Instructions - Exposed Household Members, Spanish
General Information on COVID-19, Department of Public Health, LA County
- General Information
Updated info to be added
CDC Webinar
- CDC Webinar with Micheal Bundesmann, who took care of the ~50 patients with severe COVID-19 in the Kirkland, WA, cluster. He gives a nice case series and his own perspectives with management. Waleed Alhazzani, who chaired the Surviving Sepsis Campaign’s (which may be a dirty word to some out there) position paper on the management of COVID-19 patients. He gives a lot of historical context for some of the management we are exploring with patients with severe COVID-19.
https://emergency.cdc.gov/coca/calls/2020/callinfo_040220.asp
Donning and Doffing
- CDC Donning and Doffing PDF
https://www.cdc.gov/hai/pdfs/ppe/ppe-sequence.pdf
- HIPPOED Donning and Doffing Video (4th and 5th videos)
https://covid.hippoed.com/#watch
MAXAIR CAPRS
https://www.maxair-systems.net/ProductTrainingVideos/Helmet_Basics/Helmet_Basics_A.html
Guidelines for Safe Intubation (Life in the Fastlane)
McGrath Video Laryngoscope
- How to use the McGrath video laryngoscope
https://hcpresources-en.medtronic.ca/intubation/mcgrathtm-mac-video-laryngoscope-mac-3-instruction
Ultrasound and COVID
- youtube videos cannot link to WikEM.
RSV Bronchiolitis and Other Peds Respiratory Illnesses
Waiting Room
- HR and Pulse ox will be obtained on all QR kids with respiratory complaints; completed by NA or ICN
- ED 4 Attending is responsible for monitoring how many Peds patients waiting to be seen; ED 4 Attending will tell ED residents when they need to start picking up patients. RME NP will help be the eyes/ears and let the ED4 Attending know if kids start to back up to ensure ED residents are engaged on seeing them too.
Treatment
- Suction Snot!!
- Remember, beta agonists and steroids have not been shown to helpful for kids with bronchiolitis.
Admissions
- Pediatrics will try to keep more kids here at OVMC on HFNC. Will be evaluated on case by case basis. Will likely want the child to be observed in ED on HFNC to see if they are stabilizing.
Transfers
- See Pediatric Transfer poster in the ED provider rooms
Discharges
- Autotext/dotphrase for URI and bronchiolitis discharge instructions can be found under Maureen McCollough auto text
- Nose Fridas for babies less than 6 months are available to give to parents
Neurology
Matt's Reminders
- Please call neurology for ANY questions regarding the management of stroke patients
- All CVAs with symptoms within 8 hours should be discussed with neurology
- For acute CVAs within a 5 hour window the imaging of choice is CT angiography head with and without contrast
- Admit TIAs to medicine: we don’t send them home
- E-mail Matt with any difficult neurosurgery transfers or neurology issues. Matt's cell is posted in ED. Matt has direct contact with USC Neurosurg and is happy to help in the heat of battle
Acute Stroke Protocol, Large Vessel Occlusion and TeleStroke iPad
- updated April 2025
- For suspected or presumed stroke with last time known to be at baseline ≤ 8 hrs before presentation
- Stroke Alert Background: Intent of this protocol is to create a rapid, collaborative care model for the acute stroke patient. The ED Attending or primary team attending (for non-ED patients) retains ultimate responsibility for the care of the patient and any decision-making regarding that care.
- Code Stroke pager on Quick Order/Place Order page in First Net. If no response, Stroke Alert pager number is 818-226-4797. Any physician involved in the patient’s care can activate a Stroke Alert by calling the page operator, requesting a page to the “Stroke Alert Pager,” and provide a call back number. The number can also be text paged from www.amion.com or www.myairmail.com (American Messaging). The pager is used to alert appropriate group members to a potential acute stroke in-house or in the ED. The Stroke Alert pager notifies the following staff members:
- Neurology Resident on-call
- Stroke Fellow
- ED Pharmacist
- please enter the full 10 digit call back number and add *911 or “stroke alert” to note high acuity.
ED Actions
- Page Code Stroke. (or dial 818-226-4797 or text page this number through www.amion.com or www.myairmail.com (American Messaging)).
- Briefly discuss the case with the on-call Neurology Resident. Have the symptoms and last known well time ready.
- Studies:
- CBC, BMP (including BUN and creatinine), LFTs, troponin, PT/PTT/INR
- Chest x-ray
- EKG
- Brain imaging: Discuss with the Neurology Resident and Stroke Fellow. Generally:
- STAT Non-contrast CT head AND CT angiogram head and neck if there is no contraindication to contrast
- Prepare for STAT imaging. Neurology team will coordinate with Radiology to ascertain the most suitable mode and location of imaging, including determining if MRI would be more appropriate.
- If patient meets criteria for thrombolytics or thrombectomy, the Neurology Resident will come evaluate the patient. The Stroke Fellow will assist by phone/telemedicine until the Resident (who may be off campus) arrives. SEE BELOW FOR TELE STROKE IPAD INSTRUCTIONS.
- 'IS THIS INFO HERE STILL TRUE??? I took out a line that mentioned the LVO that us involving UM to contact Holy Cross since it's listed below and the workflow has now changed' The Stroke Fellow will assist arranging for tPA or Transfer, if appropriate. In these cases, please assist by paging “tPA Case” or “Stroke Transfer,” to 818-226-4797 though www.amion.com. Texting these messages will mobilize the appropriate team.
Potential Thrombolytic Case - last at baseline <4.5 hours prior to presentation
- Text "tPA case" to 818-226-4797 and to stroke fellow, pager 818-226-4885
Large Vessel Occlusions (LVOs) at OVMC
- Mechanical thrombectomy in patients with LVOs are considered in patients presenting with deficits within 24 hours.
- The decision on which patients are candidates for a cerebral angiogram which is the first step in an intervention for an LVO is a complex decision made by the neurology team.
- The OVMC neurology resident decides with the stroke attending and/or stroke fellow if the patient is a candidate for an LVO intervention. This involves the interpretation of the CT perfusion study and CT angiography as well as the patient's presenting symptoms.
- If the patient is a candidate for an LVO intervention the STROKE NEUROLOGY TEAM ARRANGES TRANSFER TO HOLY CROSS which is contracted with DHS to provide this service to OVMC.
- Holy Cross contracts with an ambulance company; Holy Cross arranges transportation; do not call 911; do not call MAC
- UM can be notified of transfer so they can inform the health plan if patient is OOP. UM does NOT arrange transportation.
- Holy Cross may need to talk to ED team about additional medical management, e.g. need to intubate, need to correct electrolytes.
Tele Stroke iPAD instructions
- When the iPAD is receiving an incoming call, you will hear a tone.
- 1. To receive the call, please unlock the home screen (code: 800000)
- 2. Click on the blue HipaaBridge icon.
- 3. Video should start automatically.
- Receiving a call: iPAD will ring when someone is calling in.
- 1. Home screen, unlock by pressing the button (under the finger in the picture)
- 2. Press “800000” on the touchscreen to unlock the iPAD
- 3. Answer call (green button, under finger)
- Troubleshooting:
- No volume: volume tabs are on your right as you face the screen, towards the top
- Not turning on: ensure iPAD is charged. Charging port is at the bottom of the iPAD. Power button is on the top of the device, towards your right. Charging cables are stored behind the device in the locked cabinet where the iPAD is stored.
- If you wish to dial out from the iPAD (generally will not be necessary), in order to log into Hipaabridge, it may ask you for a 4-digit passcode
- If you get to this screen, and absolutely have to log in (not needed to answer a call, only needed for dialing out), press “3104” on the touch screen. DO NOT press “cancel” - this will lock the device out of HipaaBridge and currently for security purposes, only IT personnel can log back in. They can be reached at x73239 or room 1D132.
- If completely locked out from HipaaBridge and you see a log in screen requesting an e-mail or single sign on, please contact IT at x73239 or room 1D132. Currently, only they can log back in if the iPAD is completely locked out.
Neuro Clinic Referral Guidelines
- Stroke/TIA
- TIA. In general, all patients who present with a history suggestive of TIA should be admitted for risk factor assessment. Due to the high immediate risk of ischemic stroke following a TIA and the inefficiencies of outpatient diagnostic testing, inpatient monitoring and assessment ensures comprehensive evaluation and the potential for timely intervention if indicated.
- Hemorrhagic stroke. In the event of a parenchymal, subdural or subarachnoid hemorrhage, a transfer to LAC+USC should be arranged. The only exception is a parenchymal hemorrhage with symptoms already for more than 5 days, in which case admission to Olive View is permissible.
- Ischemic Stroke. All ischemic stroke patients should be evaluated by the Neurology Service. The timing of consultation shall be determined by the duration of symptoms.
- 0-3 hours: Consultation should occur in the Emergency Department to determine eligibility for intravenous tPA.
- 3-6 hours: Consultation should occur in the Emergency Department to determine eligibility for possible transfer to UCLA for intra-arterial tPA.
- 6-48 hours: Consultation should occur in the Emergency Department to help determine the appropriate level of care for admission.
- 48-72 hours: Consultation may be sought after admission (unless symptoms have progressed in a stepwise pattern or if the patient has multiple increasing, stereotypic TIA symptoms, in which case consultation should occur in the Emergency Department). Patients should be admitted to the intermediate care unit or standard care telemetry ward for 24 hours of observation/monitoring.
- >3 days: Consultation may be sought after admission. The level of care for admission is left to the discretion of the DEM attending.
- Studies to be obtained prior to Neurology Clinic consultation:
- If old, check for MRA of neck or Doppler, echocardiogram, MRI brain
- Labs: RPR, ESR, HbA1c, PT/PTT or INR, homocysteine level
- Seizures
- Patients with established epilepsy do not need consultation following a solitary seizure, if an obvious reason for the breakthrough exists (e.g., non-compliance with meds, concomitant illness). If the patient has had a 20% increase in seizure frequency in the recent past, then a request for an earlier appointment may be submitted if the patient’s scheduled visit to Neurology Clinic is >1 month into the future. Patients who have run out of anticonvulsant medication(s) may be given a supply to cover them until the next scheduled Neurology Clinic visit. If an appointment does not exist, then a 5-month supply should be given and a Request for Outpatient Consultation form submitted. If a patient has a stable seizure disorder (no seizures on anticonvulsant medication with the past half-year or more) there is no clinical necessity that the Neurology Service follow them. Medication may be refilled by Primary Care. Stable seizure patients who cannot obtain Primary Care can be most efficiently followed in one of Neurology’s Nurse Practitioner clinics.
- Studies to be obtained prior to Neurology Clinic consultation:
- Anticonvulsant levels
- EEG
- Brain MRI
- Headache
- Patients with established migraine headache who have failed primary-care attempts at management may be referred to the Neurology Clinic. Patients given a new diagnosis of migraine by Primary Care, Medical Walk- In or the DEM, who have not yet had reasonable attempts at management (use of triptans and/or appropriate preventive medications) should be referred to Primary Care prior to seeking specialist care.
- Studies to be obtained prior to Neurology Clinic consultation:
- If DEM referral, the patient should be referred to Primary Care first. If referral from Primary Care, and headache of long duration (>1 year), documentation of prior management attempts.
- Medication history
- If patient > 50 years old, ESR
- Documented neurology examination (to help determine the urgency of the referral).
- If focal findings on neuro exam, neuroimaging results or at least a request submitted for MRI of brain.
- Dizziness - In all cases of “dizziness”, Neurology is best equipped to help patients who exhibit vertigo and/or disequilibrium accompanied by focal neurological signs. Episodic light-headedness and chronic dizziness are generally better served by Primary Care, Cardiology, or Head and Neck Surgery.
- Peripheral neuropathy
- Studies to be obtained prior to Neuromuscular Clinic consultation:
- If painful, medication history
- Labs: B12, RPR, TSH, HbA1c, ESR, and consider SPEP, ANA
- EMG/nerve conduction velocities if available
- Studies to be obtained prior to Neuromuscular Clinic consultation:
- Muscle Disease
- Studies to be obtained prior to Neuromuscular Clinic consultation:
- Labs: CPK, ESR, TSH, ANA
- EMG
- Studies to be obtained prior to Neuromuscular Clinic consultation:
- Dementia
- Studies to be obtained prior to Memory Disorders Clinic consultation:
- Do not refer to General Neurology; refer to Memory Disorders Clinic
- Labs: CBC, B12, TSH, RPR, MHA-TP, Ca, Na, ALT, AST, BUN, creatinine, homocysteine, RBS Vitamin D level, lipid panel
- MRI of Brain with Dementia Protocol
- Studies to be obtained prior to Memory Disorders Clinic consultation:
- Multiple Sclerosis
- Studies to be obtained prior to Neurology Clinic consultation:
- MRI brain and/or spinal cord with contrast if available
- Labs: ANA, B12, RPR, Vit D level, ESR, SSA, SSB, consider HIV
- LP if available, for oligoclonal bands, IgG, IgG synthesis, and routine protein glucose, cell counts, differential
- Studies to be obtained prior to Neurology Clinic consultation:
Sleep Study
- Econsult Sleep Study
- Do NOT place order for sleep study; econsult should be placed but seriously ask yourself WHY AM I ORDERING THIS FROM THE ED??
DMV Request for Re-Examination Form
http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/DMV%20Request%20for%20Reexamination%20Form.pdf
Neurosurgery
A few pointers
- All transfers through the MAC are classified as “routine” or “urgent/emergent”. The language with them really matters. MOST of our transfers are ROUTINE as long as it is not immediately life threatening (e.g. stable subdural hematoma), but routine transfers can sometimes take hours. If you have a transfer from the ED such as a head bleed, and the patient decompensates while the patient is waiting for a bed at LAC-USC, the transfer actually gets easier. You can upgrade the transfer to EMERGENT through MAC and they will get you in touch with the LAC-USC DEM attending who based on our agreement will accept the patient.
- Similarly, for a CRITICAL neurosurgical patient, these transfers should be deemed EMERGENT with MAC and will be readily accepted attending to attending either by the neurosurgery attending or USC DEM attending regardless of bed status.
- For a neurosurgical transfer not going smoothly, MAC is easily able to get the LAC-USC neurosurgery attending on the phone and you can have a magical attending to attending discussion. In our experience this usually results in a satisfactory result, and they do not mind being called.
- Finally, we had a recent attempted neurosurgical transfer to UCLA. Unfortunately, ONLY ACUTE STROKE patients eligible for a mechanical thrombectomy by neurology will be accepted at UCLA from DHS hospitals. Neurosurgery transfers should go through MAC to a county facility, unless they are out of plan (OOP), in which case we should try to transfer to someplace within their plan.
Neurosurgery Transfer Guidelines
- Approved by DEMs at OVMC and LAC, LAC+USC Neurosurgery, OVMC Medical Admin and MAC Feb 2018
- If patient is OOP but stable, contact UR x74890 to attempt transfer within the patient's health plan
- For unstable or DHS/uninsured patients, transfers will be made through the MAC to LAC+USC neurosurgery (Harbor is no longer an option)
- Indications for Potential Emergency Transfer:
- ACUTE cerebral hemorrhages, including:
- Subarachnoid hemorrhage (traumatic or spontaneous)
- Intracerebral hemorrhage (ICH score >0)
- Subdural or epidural hemorrhage
- Any lesion with significant mass effect (e.g. midline shift >5mm, hydrocephalus, or increased ICP with risk or concern for herniation)
- Acute or subacute spinal cord or cauda equine compression (e.g. abnl exam with sensory level, motor deficit, or MRI evidence of cord compression with CSF block or abnl cord signal)
- ACUTE cerebral hemorrhages, including:
- Emergency Transfer may NOT be Indicated:
- Mild traumatic brain injury (no or trace blood, no fracture, GCS ≥ 14 with stable scan)
- Space occupying lesion with minimal mass effect: midline shift <5mm, no concern for herniation or increased ICP
- Chronic mild spinal cord compression - no neurological deterioration without cord signal change or CSF block around cord
- Chronic subdural hematoma (no acute blood products, size <7mm, no midline shift, no recent change in size if prior imaging available)
- How to Transfer:
- Contact LAC+USC Neurosurgery Resident to discuss case via MAC (866-940-4401); if no response, page resident directly through AMION (Logon = LACUSC)
- If no response or disagreement with NS resident, Call LAC Neurosurgery Attending (Amion logon = LACUSC; if no response or disagreement with NS Attending, call Matt Waxman 310-497-7113 or Greg Moran 818-426-1478 or LAC Neurosurgery Service Chief Dr. Arun Amar (pager 213-508-0000) or the LAC CMO of the day via MAC
- If no immediate neurosurgery intervention planned but needs monitoring in Neurocritical Care ICU, contact LAC+USC Neurocritical Care Attending (Gold Service) via MAC (866-940-4401)
- If transfer is delayed, may initiate ED to ED transfer
- If patient acutely demands urgent/emergent transfer but no DHS beds are available, page OVMC CMO on-call @747-210-3000 to obtain approval for transfer to nearest trauma or comprehensive stroke center
- Once transfer is accepted, call Utilization Management (UM) at 74890. Notify them of the accepting facility and accepting physician. UM will then take the lead in the transfer process.
- How to Handle if Transfer maybe NOT indicated:
- Contact LAC Neurosurgery via MAC (866-940-4401) to discuss patient's case
- If no indication for emergent Neurosurgical intervention or ED to ED transfer, may call LAC+USC Neurology Gold Service or Medicine via MAC
- If no indication for emergent transfer to LAC+USC Neurology or Medicine, may undergo initial evaluation and treatment at OVMC
- Re-evaluate transfer if imaging or condition worsens
OB-Gyn
Referral Guidelines for Message Pool vs Econsult
- Urgent Followup through Message Pool in Cerner/Orchid
- These go to NP clinic and will be seen usually within a few days
- First trimester vag bleed
- Complicated PID that needs GYN followup
- AUBs who are anemic (hgb less than or equal to 9)
- Post menopausal bleeding
- Bartholyn's cysts
- Labial abscess
- These go to NP clinic and will be seen usually within a few days
- Econsult to GYN
- These go to an MD clinic and will usually be seen in 2-4 weeks
- AUBs with stable hemoglobin
- Ovarian cysts
- Chronic pelvic pain
- Urogyn
- These go to an MD clinic and will usually be seen in 2-4 weeks
Establishing care at OVMC for pregnant patients
- Do not refer OOP patients; refer these back to their health plan
- For uninsured patients, tell patient to go to Clinc D to request follow-up for pre-natal care, "PK" clinic; clinic closes at 4pm
- REMEMBER, use Message Pool for an urgent request for pregnant vag bleeds, rule out ectopics getting BHCG checks, etc
Oral Contraceptive Taper Patient Instructions
http://myladhs.lacounty.gov/ov/Departments/OBGYN/Documents/PtInfoCounseling/GYN_Combined_OCP_taper_English.pdf http://myladhs.lacounty.gov/ov/Departments/OBGYN/Documents/PtInfoCounseling/GYN_Combined_OCP_taper_Spanish.pdf
Oral Provera Taper Patient Instructions
- Coming soon!!
Ordering Rhogam
- In Cerner, order "RhIG Request"; right click on order to modify order, 300mg,intramuscular, prenatal
Ophthalmology
Ophthalmology Abbreviations
AAU: acute anterior uveitis AFT: artificial tears AGV: Ahmed glaucoma valve ARMD or AMD: age-related macular degeneration DR: diabetic retinopathy BRAO: branch retinal artery occlusion BRVO: branch retinal vein occlusion BULB: bilateral upper lid blepharoplasty BVS: borderline visually significant C/D: cup-to-disc ratio CEIOL: cataract extraction with insertion of intraocular lens CME: cystoid macular edema CRAO: central retinal artery occlusion CRVO: central retinal vein occlusion CSME: clinically significant macular edema CS: cortical spoking (cataract) CSR: central serous retinopathy DES: dry eye syndrome DME: diabetic macular edema DWC: dense white cataract ED: epithelial defect EL: endolaser ERM: epiretinal membrane FML: focal macular laser GS: glaucoma suspect HST: horseshoe tear HVF: Humphrey visual field K: cornea KP: keratic precipitate (inflammatory cellular deposits) LH/WC/AFTs: lid hygiene, warm compresses, artificial tears LPI: laser peripheral iridotomy MMCR: Muller's muscle conjunctival resection MP: membrane peel NAION: nonarteritic ischemic optic neuropathy NCVH: non-clearing vitreous hemorrhage NPDR: non-proliferative diabetic retinopathy NS: nuclear sclerosis (cataract) NTG: normal tension glaucoma NVG: neovascular glaucoma NVS: not visually significant OD: right eye OHTN: ocular hypertension OS: left eye OU: both eyes POAG: primary open angle glaucoma PCO: posterior capsular opacity (aka, secondary cataract) PDR: proliferative diabetic retinopathy PKP: penetrating keratoplasty (aka corneal transplant) PPV: pars plana vitrectomy PRP: pan retinal photocoagulation PS: posterior synechiae (sequelae of inflammation) PSC: posterior subcapsular cataract PTG: pterygium PVD: posterior vitreous detachment RRD: rhegmatogenous retinal detachment RT: retinal tear SB: scleral buckle SRD: serous retinal detachment Trab: trabeculectomy TRD: tractional retinal detachment VA: visual acuity VH: vitreous hemorrhage VS: visually significant XT: exotropia YAG cap: YAG capsulotomy
Orthopedics and Podiatry
- Orthopedic Surgery and Podiatry share clinic space and communicate regarding complex lower extremity cases.
Ortho and Podiatry Clinic Referral Guidelines
| OVMC Orthopedics | OVMC Podiatry |
| Patients 16 years of age and older | Majority of foot and ankle fractures are managed by podiatry (5th metatarsal fractures, ankle fractures) |
| High Energy ankle fractures such as a pilon fracture | Diabetic foot including osteomyelitis |
| Maisonneuve fractures involving the fibular head | Ankle sprains |
| Lisfranc fractures (tarso-matatasal injury) | Plantar fasciitis |
| No acute soft tissue knee injury (non-fracture) greater than age 55 | |
| No hip fractures) (Transfer out) | |
| No compartment syndromes (General Surgery) | |
| No Open fractures (Transfer out) | |
| Tibial plateau and knee fractures | |
| Upper extremity injuries proximal to mid-forearm. (Distal to forearm goes to Hand) | |
| No septic arthritis involving history of arthroplasty (prosthetic joint) (Transfer out) | |
| Will operate on septic arthritis with fracture hardware (wires, plates) |
OVMC Pediatric Orthopedics
- Emergent Peds Ortho cases less than 16 years old, e.g. open fractures that require OR debridement, should be transferred out via the MAC for uninsured or to the patient's health plan whenever possible
- All other pediatric orthopedic cases should be referred to OVM Peds Ortho via the Message Pool. All of these cases will be reviewed by Dr. Farrell and he will determine if the case should stay here at OVMC or be referred to Peds Ortho at USC
- If the case needs referral to USC Peds Ortho, the Ortho clinic here at OVMC will handle the referral to USC
Pain Assessment Workflow
- If a nurse flags a patient as "pain level unacceptable, collaborate with provider" a purple ICON appears for the patient on the tracking board under the PAIN column.
- This PAIN icon will automatically go away if the provider writes for a pain medication order.
- If an order for a pain medication is not appropriate, the provider can remove the ICON by manually cancelling the Request Pain Medications order. If pain medication is not appropriate, it should be documented in the chart by the provider.
ED Pain Assessment Workflow Job Aid
ED Pain Assessment - Brief Provider Job Aid
Pediatrics
- Pediatric attending should be notified for any pediatric patient transferred out
- Pediatric patients (non-OOP) can be told to return to the Pediatric Urgent Care clinic for follow-up issues
- For any pediatric patient requiring follow up with a subspecialist (non-OOP), contact the Pediatric Attending on-call as needed for any questions regarding follow-up
Pediatric Subspecialists On-Call
Pediatric Transfers / Critical Pediatric Patients
Peds patients seen in ED
- Peds Resident pager 818-313-1739 Also available through Cerner...Consults Auto Paging OVMC
- Weekdays: 0800am-3:30pm Triage RN should contact Super Track Attending or NP to screen patient (ESI 3-5) as OK to go to Peds Clinic. MSE note should be completed. Parents are given map and walk to Peds Clinic.
- If patient is roomed in the ED, page Peds Resident
- Weekdays: ED sees peds patients until 10am
- Overnights, Weekends, Holidays: Pediatric Resident and Emerg Med Resident will share patients. Peds residents will see bulk of patients after hours until 2am. ED residents can also see patients when there are multiple pediatric patients to see.
- At 2am, ED residents will see pediatric patients until 10am the next day
- DEM PROVIDERS SHOULD CALL PEDS EARLY for any pediatric patient that is likely to be admitted
Bilirubin Babies
- Weekend Outpatient Bilirubin Lab Draws for Neonates - Guidelines from Dept of Pediatrics
- Inform the caregivers that their infant needs a lab draw on Saturday or Sunday. Please remind the caregivers that this is a critical lab value and they should arrive at Olive View lab by 10:00AM.
- Obtain contact information for caregivers and document in the most recent note:
- Phone number
- Home Address
- Instruct caregivers to go directly to the lab on either Saturday or Sunday, as clinically indicated. The lab does not require messaging, paperwork, or notification.
- Olive View Laboratory
- Location: Room 1A140
- Phone number: 747-210-4039
- Hours: 8:00AM – 12:00 NOON on Saturday and Sunday
- Please go directly to the lab. You do no not an appointment or paperwork. Lab doors unlocked at 8am.
- Olive View Laboratory
- Order total and direct bilirubin labs STAT. Be sure to select nurse collect: NO and order for future visit: YES. Set the collection date and time to your anticipated date and time. Add the weekend pediatric inpatient attending as the “Attending Physician” in the bottom right of the lab order.
- Give a sign-out / warm handoff to the pediatric inpatient wards attending, including:
- Caregiver contact information
- Clear “to-dos”
- The inpatient attending will add the patient to the electronic Float Book. The attending will inform the weekend senior resident of the expected bilirubin result over the weekend.
- The on-call senior resident will follow-up the bilirubin result and call the pediatric inpatient attending to discuss plan of action. The on-call senior resident will then call the family to provide the plan of care and document a telephone encounter note. If the lab has not resulted by 2PM, the on-call senior resident will follow-up with the lab and the family.
- Inform the caregivers that their infant needs a lab draw on Saturday or Sunday. Please remind the caregivers that this is a critical lab value and they should arrive at Olive View lab by 10:00AM.
Child Maltreatment/Non-Accidental Trauma/Sexual Abuse
- OVMC HUB/SCAN Clinic
- OVMC has its own HUB/DCFS Clinic on campus over in the Women/Children's building. phone x74680
- This clinic sees children who are victims of both non-accidental trauma and sexual abuse.
- Staff includes specialized pediatricians, social workers, DCFS case workers, and nurses
- OVMC HUB Clinic can see patients regardless of their insurance status, including outside health plans.
*Monday-Friday, 8am-8pm: Call the OVMC HUB Clinic x74680
*NOTE: HUB CLINIC DOES NOT TAKE OVER THE CARE OF ACUTE CASES. ED IS STILL RESPONSIBLE FOR REPORTING CASES TO DCFS, CONSULTING SOCIAL WORK OBTAINING ANY ADDITIONAL IMAGING OR LABS NEEDED. HUB CLINIC IS AVAILABLE FOR FOLLOW UP!
*After-hours, weekends, holidays:
- Notify the pediatric resident on-call and the Pediatric Attending on-call
- Place Consult to Social Work; place consult early so they can be present when the parent/caretaker/child is giving the history
- THE PROVIDER (EITHER CLINICAL SOCIAL WORK STAFF OR PHYSICIAN) WHO TAKES THE HISTORY SHOULD BE THE ONE WHO CALLS DCFS TO REPORT THE CASE
- When Social Worker is not present, they will come in for serious child abuse cases/deaths After Hours Pager (818) 313-1637
- Peds Attending will know who from the Dept of Pediatrics is on call for child abuse cases.
- Peds Attending/HUB Clinic Attending on-call will guide management re: what needs to be done in the ED in regards to labs or imaging and will help get the child scheduled in our HUB Clinic for follow-up. Peds Attending/HUB clinic attending will help decide if case is URGENT or NON-URGENT.
- See below for how to handle URGENT vs NON-URGENT cases
URGENT CASES
- Step 1: Report case to DCFS (Dept of Children and Family Services); can be done by SW or provider
- NOTE - WHOEVER TOOK THE HISTORY SHOULD BE THE ONE TO CALL DCFS; CALL CLINICAL SOCIAL WORK EARLY TO BE INVOLVED
- Phone - (800) 540-4000
- You will be given a 19-digit Referral/Case Number that you will need when completing the on-line form. Please document the 19-digit referral/case number in the patient's chart.
- Step 2: Fill out on-line SCAR (Suspected Child Abuse Referral) form. You MUST have the 19-digit Referral/Case Number in order to complete the on-line SCAR form; it may take up to 2 HOURS for the referral/case # to be activated by DCFS. After you complete the on-line SCAR form, you will get a 16digit tracking number; please document this in the chart. Please PRINT OUT the SCAR form, give it to clerk to upload into chart.
- On-line SCAR form link: https://mandreptla.org/cars.web/CallType
NON-URGENT CASES
- Step 1: Peds Attending/HUB Clinic Attending can help decide if case is ok for non-urgent reporting. If pt is <2 yrs old, use URGENT report process.
- Use the CARES on line form to report non-urgent cases. https://mandreptla.org/cars.web/
- CARES on line form has 10 questions that must be answered to determine if case is appropriate for non-urgent reporting.
- For pediatric sexual assault, do not perform a detailed history or exam. History and exam should be brief, just to determine if a medical emergency exists.
After Hours: LA General or Northridge CATS
- HUB Clinic Attending may say that a child needs to be seen that night or on the weekend. We use LA General HUB Clinic or Northridge CATS clinic. Patient will go with law enforcement. Document law enforcement office name, bade # in the chart. Law enforcement will often decide which center they will take the patient to. We encourage LA General because follow-up is easier. CALL LA GENERAL OR NORTHRIDGE AHEAD OF TIME and DOCUMENT WHO YOU SPOKE WITH.
LA General HUB Clinic. 323-409-3601. Ask to speak to Peds Attending who will know HUB clinic provider on-call.
Northridge CATS (Center for Assault Treatment Services) (818) 908-8630 or (818) 908-8632.
Plastic Surgery
Upper Extremity Splinting Recs
OVMC Upper Ext Splinting Recs.pdf
Psychiatry
- x74340
- For patients without medical complaints, medically screen patients at Triage or Ambulance Triage. If medically cleared, nursing calls for nurse to nurse report. ED provider only needs to call if unusual case or ED provider has a question. Otherwise provider to provider call not necessary.
- If patient is placed into an ED bed and needs emergent psychiatry, order Consult to Psychiatry and call x74340 to speak to Psychiatry MD.
Olive View Mental Health Clinic
- located behind the hospital
*As of April 2025, clinic now will see walk-in patients for medication refills during their business hours.
- patients will be tested for COVID as they are in a shared waiting space
- operated by LA County Dept of Mental Health
- 818-485-0888
- hours M-F 8am-7pm, Sat 9am-5:30pm, closed Sundays and holidays
- Able to see patients with outside health plans (OOP)
Can I place a patient on an "8 hour hold" like at UCLA?
- No, we cannot use the Calif law 1799 that allows non-LPS designated facilities/hospitals to place psychiatric patients on an 8-24 hour hold until the patient can be evaluate by a psychiatric team that must come from the outside.
- LPS stands for Lanterman-Petris-Short Act which allows psychiatric patients to be placed on involuntary holds for 72 hours, etc (e.g. 5150)
- LPS designated facilities are allowed to receive 5150 patients by EMS, police and accept transfers; LPS designated facilities have psychiatric providers on-site
- OVMC, Harbor, LA General, Northridge, Glendale Memorial, and others are LPS designated and therefore CANNOT use 1799 to hold patients before psych places them on a hold
- UCLA NPI is a LPS designated facility also
- UCLA RR is technically NOT an LPS designated facility and therefore CAN use the 1779 law to hold patients until psychiatry comes to see them.
- What we can do at OVMC:
- 1. If patients are brought in by police, if possible, insist that the police write the hold if the patient said to police "I want to kill myself", police found pt standing with noose around his neck, etc. Officers are often resistent to writing the 5150s and we need to insist more often that they do. Blank 5150's are at the charge nurse chair/desk in the forms rack on the left.
- 2. place 1:1 sitters on patients
- 3. If patient will cooperate, have patient change into a gown. If patient bolts out the door, much easier to spot them wearing a gown. Don't fight the patient on this issue though. Please avoid agitating the patient.
- 4. Call psych early
- 5. Check in with patient often to update them on the wait for psych
- 6. Feed patients
- 7. Use Xyprexa earlier to decrease chance of patient escalating
- 8. If you are worried a patient may bolt and psych has not seen the patient yet, you can call psych back and state you have a "psych emergency" and you need them "stat". There is an agreement between the departments that psych will come immediately if we say it's an emergency assuming they are not already dealing with an emergency on their end. Please use this judiciously. We don't want the "boy who cried wolf" problem.
- 9. If the patient does leave and you felt the is concern enough for the patient to be on a 5150, call the Sheriff. If you believe the patient was likely to be put on a 5150 hold, make sure the Sheriffs know this. They are not allowed to just bring the patient back just because we say so. They will go look for the patient, engage the patient, and if the patient says or does something that is concerning for SI/HI/gravely disabled, then the Sheriffs can bring them back. More often than not the patient is brought back. The Sheriff is very good about engaging these patients well.
Radiology
On-Call Radiologist and In-House Radiology Coverage Schedule
- Operator has Radiology on-call schedule and pager numbers
- Also posted on OVMC Website...Departments....Radiology....On-Call Schedules....Radiology Faculty Schedule Current Month
- https://lacounty.sharepoint.com/sites/dhs-ov-radiology/Radiology%20On%20Call%20Schedules/Forms/AllItems.aspx
On-Call Tech Supervisor Schedule
- Also posted on OVMC Website...Departments....Radiology....On-Call Schedules or Radiology Schedules....current month Supv and Techs On-Call schedule (link below_
- https://lacounty.sharepoint.com/sites/dhs-ov-radiology/Radiology%20On%20Call%20Schedules/Forms/AllItems.aspx
In House Coverage
- M-F 6 pm-10 pm: STAT OVMC Radiology Attending in-house
- M-F 10pm-06:30am: STAT RADS or US ROC (see After Hours Coverage)
- Sat, Sun Holidays before 1pm: General Radiology Attending in-house
- Sat, Sun, Holidays 1p-7 pm Sat: STAT OVMC Radiology Attending in-house
- Sat, Sun and Holidays 7pm-7am: STAT RADS or US ROC (See After Hours Coverage)
StatRad Coverage for CT and MRI Overnight and Weekend Reads Only
- StatRad coverage Mon-Fri 10pm - 0630am and Weekends/Holidays 7pm-7am
- StatRad will fax the prelim reads and the tech will scan that into Synapse. Instead of viewing in the Synapse "Notes" section you view in the "Documents" section in "Technologist Notes".
- If you would like to discuss the case with the Radiologist or you have any problems or concerns with the service, please call their reading room 858-546-3800, press 1.
- If it is not coming through you can log onto the site to check the status at https://clients.statrad.com
- The first time you log in use the temporary password "Olive" and you will then be prompted to enter a new password. Hopefully you will not have to use the portal at all. Only Attendings have log in IDs for now.
- Attending IDs for log-in https://lacounty.sharepoint.com/:x:/r/sites/dhs-ov-emergencymedicine/_layouts/15/Doc.aspx?sourcedoc=%7B5400E91A-2B4F-44D4-9BAA-3280DEE276BF%7D&file=StatRad%20ED%20Physician%20accounts%20for%20UCLA%20OV.xlsx&action=default&mobileredirect=true
- Website access instructions https://lacounty.sharepoint.com/sites/dhs-ov-emergencymedicine/Shared%20Documents/Forms/AllItems.aspx?id=%2Fsites%2Fdhs%2Dov%2Demergencymedicine%2FShared%20Documents%2FDocuments%2FStatRad%20Exam%20Status%2Epdf&parent=%2Fsites%2Fdhs%2Dov%2Demergencymedicine%2FShared%20Documents%2FDocuments
USROC Coverage for Ultrasound Overnight and Weekend Reads Only
- Monday-Friday 10p-06:30am and Weekends/Holidays 7p-7a
- 866-448-7762
Over-Reads
- Urgent or Emergent?
- Radiology to call x3649 or x4938 and report to ED Attending
- ED Attending shall document in the........TBD
- Non-Urgent?
- Radiology to email patient name, MRUN, date of study, and findings to Ari Orue NP at aorue@dhs.lacounty.gov
Film Copy Request and Outside Film Imaging Upload
- Film Copy Request
- Tell ED clerk that you need patient films copied onto a CD
- ED Clerk will complete the Radiology Request form and handle the request with Radiology
- Monday - Friday 8am-11pm: Release of Information (ROI) Unit, 1B114
- After 11pm, weekends and holidays: ED Radiology
- Request Form also available on the OVMC Intranet...Departments....Health Information Management...Radiology Forms
- Outside Film Imaging Upload in Cerner
- Tell ED clerk that you need patient imaging CD uploaded into Orchid/Cerner; give ED clerk the CD
- ED Clerk will complete the Radiology Request form and handle the request with Radiology
- Monday - Friday 8am-4:30pm: General Radiology 2D141
- After 4:30pm, weekends, and holidays: ED Radiology
- Request Form also available on OVMC Intranet...Departments...Health Information Management...Radiology Forms
Plain Films and No Need for Pregnancy Tests
- July 2016 - In a discussion with Dr. Patel from Radiology and Mike Ruiz, Sup Rad Tech, it was re-affirmed that women do NOT require a pregnancy test prior to plain film X-rays
- Under protocol, Radiology techs will ask the patient if she is possibly pregnant and the date of her LMP period (should be within the last 4 weeks).
- As per the American College off Radiology and the OVMC Dept of Radiology: If a patient can reliably answer that 1) she cannot be pregnant (for example, she is not sexually active, or she is using an effective form of birth control, or she is biologically incapable of conceiving) and that 2) she had a recent complete menstrual period, then it is reasonable to proceed with a medically indicated diagnostic X-ray test of the abdomen or pelvis. The last complete menstrual period should have occurred within the previous 4 weeks.
- Prior to CT scans, a pregnancy test should be obtained as the amount of radiation is higher. If, however, the patient's medical condition could deteriorate and the CT scan is needed emergently (e.g. head CT for AMS), then a pregnancy test may not always be obtained prior to the scan.
Fluoroscopy
- On rare occasion, fluoroscopy might be needed to reduce a fracture or fracture/dislocation
- Fluoroscopy is available Mon-Fri 8am-4pm, call Main Radiology x74059
- After hours, availability for fluoroscopy will depend upon hospital tech availability; talk to ED Radiology tech
- Order in Cerner: RF Fluoroscopy Under 1 hour
Interventional Radiology
Protocol for Urgent Interventional Radiology Procedures
- 1. ED Provider contacts IR provider on-duty or on-call to determine the appropriate timing of the requested procedures and determine if the procedure can be done in next few days.
- a. Weekdays 8am-4:30pm: call x74554/66088/73931 to find the interventionalist on-duty or Ana Barajas DNP. Also available on OVMC Intranet…..Search: Radiology Schedules...Faculty Schedule.
- b. After Hours: Operator has Interventional Radiology on-call schedule. Also available on OVMC Intranet....Search: Radiology Schedules....Faculty Schedule.
- c. See below for Interventional Radiology procedures available after hours
- 2. If patient is on anticoagulant, IR provider on-duty or on-call will determine whether or not anticoagulants need to be held and for how long.
- 3. If procedure can be scheduled for the next business day or two, ED Provider obtains pre-procedure labs/studies including COVID-19 testing as requested by the IR provider on-call . COVID-19 testing should be ordered as Admit Asymptomatic.
- 4. ED Provider places an order in Cerner for the desired procedure, indicating FUTURE ORDER:
| Issue/Problem | Order in Cerner |
| Dialysis fistula not working/declotting | IR angiogram arteriovenous shunt |
| Tunneled catheter needed | IR central venous catheter tunneled |
| Exchange nephrostomy tube | IR Exchange of nephrostomy catheter |
| G-Tube change | IR Gastrointestinal Tube or Catheter Change |
- 5. ED Provider sends a message through ORCHID using IR Message Pool: OVM - IR - PROVIDERS. ED Provider will document name of IR Provider who approved procedure and time frame, e.g 1-2 days.
- 6. ED Provider gives patient a Patient Education/Discharge Instructions including NPO after midnight except for medications with sips of water. Directions regarding anticoagulants should be answered by IR Provider on-duty or on-call.
- 7. DC Instructions located in Cerner...Patient Education.....Departmental.....Outpatient Followup Interventional Radiology Procedure (English and Spanish available).
- 8. Patient is to arrange transportation to and from OVMC on the day of the procedure.
- 9. IR Provider will tell ED provider when the patient is to show up for the procedure; patient is to report to OSPA 2B-121 on the day of procedure (This may be subject to availability of OPSA beds).
AVAILABLE and NOT AVAILABLE Interventional Radiology After Hours
- (Operator has Interventional Radiology on-call schedule. Also available on OVMC Intranet under Radiology On-Call Schedule. Also available on Amion...OV IM....All Services)
- AVAILABLE
- Percutaneous abscess drainage
- Image-guided paracentesis
- Image-guided thoracentesis
- Percutaneous cholecystostomy
- Percutaneous nephrostomy/nephroureteral stent placement and other urologic intervention as applicable
- Transhepatic biliary drainage and other biliary intervention as applicable
- Central venous access including placement of tunneled/non-tunneled catheter
- IVC filter placement
- Transarterial embolization for unremitting hemorrhage refractory to conventional therapy
- IR Consultation
- NOT AVAILABLE Interventional Radiology After Hours (Only available Mon-Fri 8am-5pm)
- No MSK procedures (e.g. no joint aspirations)
- No LPs
- No G/GJ tube replacement (if tube fell out, place foley temporarily)
Dialysis AV Fistula Evaluation
- For evaluation for flow, order "US Duplex Hemodialysis Access Flow"
- For de-clotting by IR, order "IR Angiogram Arteriovenous Shunt"
MRI After Hours
- MRI tech is in-house Mon-Fri 7am to midnight. All other hours are considered off-hours.
- MRI tech is on-call for emergent cases limited to acute cord compression and rarely acute CVAs if requested by the Neuro Service for patient management (e.g. large CVA that may be considered for transfer to UCLA for intracerebral angio therapy)
- Findings that suggest acute cord compression include:
- 1. Bladder dysfunction (urinary retention or incontinence)
- 2. Bilateral limb weakness
- 3. Sensory abnormalities with a sensory level
- 4. Flaccid areflexia with upgoing toes, loss of anal sphincter tone
- Some cases may be able to wait until the morning hours such as IVDA, fever and back pain without neuro findings.
- To request an emergent MRI when the tech is not here, first contact the STAT Radiologist in-house Mon-Fri until 11pm and weekends/holidays until 7pm. If there is no STAT Radiologist in-house (e.g. after 11pm), contact the Neuro Radiologist on standby (on-call).
- On-call schedule can be found on OVMC Intranet...Departments...Radiology...Radiology Faculty Schedule Current Month.....Neuro/MRI Standby. Operator has on-call schedule also and pager #s.
- If no STAT radiologist, ED MD pages the Neuro Radiologist on standby (on-call) and requests MRI.
- STAT Radiologist or Neuro Radiology Attending then pages the MRI tech.
- For cord compression cases, as much as possible, try to narrow down the level where the possible pathology lies e.g. lumbar vs thoracic. If this is not possible, a "cord compression" MRI protocol can be performed that will give a large field of view (sagittal images) that will cover the whole spine in two slabs (cervical through mid-thoracic and mid-thoracic through lumbar), along with axial T2 images through the whole spine. Will not give great detail, but will see gross cord compression or high grade lumbar spinal canal stenosis. Decision about what imaging is performed will be up to the Neuro radiologist on-call.
MRI for Large Patients
- Weight limits and gantry (size) limits: (Note: measure patient at widest width either top to bottom or left to right; must be able to fit into MRI scanner)
- OVMC - 350lbs and 60cm
- LAC+USC - 300 lbs and 19inches
- Harbor- one MRI: 350lb and 65cm; 2nd MRI: 450 lbs and 60cm
- Downey MRI Center, 8515 E. Florence Ave, Downey CA, 90240, 562-904-1340 (Open 7 days a week, 0630am-11pm) - 550 lbs and 17inches from top of table to scanner
- Garfield Insight Imaging Center, located at Garfield Medical Center, 555 N. Garfield Ave, Monterey Park CA, 91754, 626-572-0912 (Open Mon-Fri 7am-6pm) - 550 lbs and 74cm. Need to fax patient demographic information and order request for imaging.
- These are the manufacturers weight limits. We have to be mindful and not get too close to the limit, or the table will break
- Harbor should be considered first option if possible as they have a scanner up to 450lbs
- Our MRI techs should help expedite this; otherwise escalate to the Radiologist
- Call ANO for transportation. Patient will be sent there via ambulance and then returned via same ambulance.
- If the patient requires sedation, this will be a problem for Downey or Garfield imaging centers.
- Utilization Management can help if the patient has insurance
- Ensure a CD of the imaging is brought back with the patient if sent to Downey or Garfield and if possible have the imaging read by their radiologist also just in case we cannot upload the images
- For imaging done as an outpatient after ED discharge, order as Future Order; Patient should call OVMC MRI to schedule and OVMC MRI will then arrange the MRI at Downey
OVMC Weight Limits for Imaging
- ED xray table - 500lbs
- ED CT scanner - 550lbs* (*Note - an additional black table located in the ED CT Room can be used and the weight limit is then 650lbs)
- MRI - 350lbs
- Downey MRI - 600lbs (see MRI Imaging for Large Patients)
- Cath Lab - 500lbs
- Nuclear Medicine - 300lbs
Barium/Air Enemas for Intussception Cases
- Surgical resident on-call should be made aware of any pediatric patient who is considered to have a possibility of intussusception
- Patient should have no contraindication to a barium or air enema such as evidence of peritonitis or perforation.
- M-F Business Hours: Peds Radiologist Dr. Chawla usually performs the BEs/AEs
- M-F 6 pm-11 pm: STAT Attendings will perform any BEs/AEs during their STAT shift
- Sat, Sun Holidays before 1pm: General Radiology Attending is responsible
- Sat, Sun, Holidays 1p-7 pm Sat: STAT attendings will perform any BEs/AEs during their STAT shift
- M-F 11 pm- 7am and Sat, Sun, Holidays 7pm-7 am: General standby call is responsible for performing the BEs/AEs
UGI for Malrotation/Volvulus Cases in Infants
- As per Dr. Andrews of Radiology, we have the ability to do an Upper GI 24/7 to evaluate an infant for malrotation/volvulus
- Contact the ED Radiology tech if a study is required
Breast Mass and Infection Management and Imaging April 2023
- OOP patients should be referred back to their Health Plan/PCP.
- RADIOLOGY has protocol in place for breast imaging follow-up. They will ensure patient receives their results and they will refer patients to Breast Surgery who have concerning findings. All patients require imaging before being sent to Breast Surgery clinic.
- see attached OVMC ED Breast Complaints algorithm
Joint and Spine Injections
- Dr. Raffi Salibian x75145
- Dr. Catherine Yim x74082
- Joints:
- Order: X-ray plain view
- Future Order: US aspirate/injection/biopsy (use Relevant History to indicate which joint)
- CBC and Coags if patient is coagulopathic
- Lumbar Spine (facets and epidurals):
- Send Message Center message to Dr. Catherine Yim requesting lumbar spine injection with the name of the ED Attending requesting the procedure.
- Future Order: MRI lumbar spine (Patient must call to schedule the MRI. Radiology phone # is pre-printed on ED Patient Summary/Discharge Instructions)
- Future Order: IR facet inject lumbar (need kg weight)
- CBC, Coags please
- Radiology will contact the ED TFU Coordinator or Urgent Care TFU Coordinator through the Message Pool with any problems
Renal
Workflow to Access Dialysis
- ED calls on-call Renal Fellow for all HD/PD or potential HD initiation, regardless of reason for admission - e.g., dialysis patient being admitted for cellulitis or elective procedure, etc.
- Fellows review and discuss case and plans for possible transfer with Renal Consult Attending.
- If transfer is deemed necessary, Renal Consult Attending calls and discusses case with Dr. Chi Pham.
- Dr. Pham will work behind the scene (e.g., discuss with HD service/ANO 74586 to come up with creative/alternative plans if possible).
- Dr. Pham will then call "ED hotline" to give final plan. ED hotline number: 73648 and 73649
- In the event when Dr. Pham is not available: Renal Consult Attending discusses case and transfer plans with Dr. Jafari. *There will be one week this academic year when both Dr. Pham and Dr. Jafari will be out of town (June 23-28, 2020), in which case, Dr. Kamarzarian will make the final call regarding transfers.
Surgery
- For surgical vs medicine admissions, see Surgical Subspecialty Admissions Guidelines under Admission Guidelines.
- For ALL surgical transfers out, ED Attending needs to speak to Surgical Subspecialty Attending
911 Trauma Re-Triage
- To be used for trauma patients brought in by EMS by mistake or walk-in/drop-off patients with life-threatening traumatic injuries requiring EMERGENT (aka immediate) surgical intervention that we do not have at OVMC e.g. neurosurgical
- Other EMERGENT surgical cases such as stab wounds or GSWs should be evaluated with the consult surgical resident (and Attending as needed) on a case by case basis as many of these such as abdominal trauma may be able to be cared for here at OVMC by the Dept of Surgery
- Please, if possible, ensure the Surgical Attending on-call is aware of the case. We have transferred trauma patients out that could have been taken care of by our Surgery Dept.
- Step 1: You MUST HAVE an ACCEPTING PHYSICIAN (new EMS policy Sept 2020)
- Adult Patients
- Holy Cross, by Trauma Center policy, is OVMC's designated Trauma Center.
- Call Holy Cross, ask for Charge RN and get an accepting physician; Holy Cross ED # 818-496-3302
- Pediatric Patients, 14 yrs old or younger
- Call Northridge Hospital, ask for Charge RN and get an accepting physician; Northridge ED #818-885-5396
- Adult Patients
- Step 2: Call LAFD Emergency Transport 213-847-5340/Olive View code 575 Tell them you have a "Trauma Re-Triage" patient
- Do NOT call the MAC Center. DO NOT CALL 911.
- Copy all records and imaging but do not delay transfer
- Because of the limited scope of practice by the paramedics, if the patient has blood hanging or has any drips, then our OVMC Critical Care Transport team will accompany the patient in the EMS ambulance to Holy Cross.
- County Policy: 9-1-1 Trauma Re-Triage – This section applies to injured patients in emergency departments of non-trauma centers whose injuries were initially estimated by EMS to be less serious (under triaged) or patients who self-transported (walk-in) to a non-trauma center, and subsequently assessed by the non-trauma center physician to require immediate trauma center care. The referring facility shall utilize the procedure outlined below to expedite transfer arrangements and rapid transport to the trauma center. This process should be reserved for patients with life-threatening traumatic injuries requiring emergent surgical intervention.
- A. Determine if the injured patient meets any of the following 9-1-1 Trauma Re- Triage criteria:
- 1. Persistent signs of poor perfusion
- 2. Need for immediate blood replacement therapy
- 3. Intubation required
- 4. Glasgow Coma Score less than 9
- 5. Glasgow Coma Score deteriorating by 2 or more points during observation
- 6. Penetrating injuries to head, neck and torso
- 7. Extremity injury with neurovascular compromise or loss of pulses
- 8. Patients, who in the judgment of the evaluating emergency physician, have high likelihood of requiring emergent life- or limb-saving intervention within two (2) hours.
- B. Contact the designated receiving trauma center or pediatric trauma center if the patient is less than or equal to 14 years of age and transport does not exceed 30 min. Do not delay transfer by initiating any diagnostic procedures that do not have direct impact on immediate resuscitative measures.
- C. Contact 9-1-1 for transportation. The paramedic scope of practice (Ref. No. 803) does not include paralyzing agents and blood products.
- D. Prepare patient and available medical records for immediate transport. Do not delay transport for medical records which could be sent at a later time.
- E. EMS has no immediate solution if there is refusal by the Trauma Center; remind them of the EMS 911 Trauma Re-Triage Policy, that they are our receiving facility; please let McCollough know about any refusals
- A. Determine if the injured patient meets any of the following 9-1-1 Trauma Re- Triage criteria:
Surgery Clinic Referral Guidelines
- Econsult: All hernias and gallbladders need the hernia/chole form filled out - asks about BMI and cigarette smoking
- Surgery will not perform hernia repair or cholecystectomy if BMI >35
- Surgery will not perform hernia repair if patient smokes
- For breast cases, see WikEM OVMC:ED....Radiology....Breast imaging
Breast Issues
- For breast cases, see WikEM OVMC:ED....Radiology....Breast Mass and Infection Management and Imaging
Cardiothoracic Surgery
- We have non-cardiac Cardiothoracic Surgery at OVMC. If you have a case, consult General Surgery who will consult with Cardiothoracic Fellow/Attending
Neurosurgery
- See Transfers...Higher Level of Care....Neurosurgery
Vascular Surgery
- No update
Laboratory
Critical Lab Results on ED patients, ED Boarders (Admitted Patients), and ICU patients
- Lab tech will determine if a patient is an ED patient or an ED Boarder prior to calling a critical lab result. Lab techs have a cheat sheet that outlines this process.
- ED patients: critical lab report goes to ED provider or attending. Lab tech should contact ED provider in the provider room based on patient location (main ED room or SuperTrack room. Lab has been given a list of ED patient rooms and the MD Room associated.
- ED Boarder/Admitted patients: Lab tech should call the ED nurse directly based on patient location in the ED. Nurse will forward results to the inpatient team.
- All ICU patients: Lab tech should contact the ED provider directly for all critical labs on ICU patients since ICU boarders are still managed by the ED team.
Critical Lab Results on Discharged ED Patients
To be added
Infrequent Lab Orders - Instructions
Rapid Strep
- Order as Rapid Strep Group A Ag. Do NOT order POC Rapid Strep.
- Run 24/7 when the test is received in the lab. General turnaround time 30mins.
Varicella Testing
- For Varicella testing,VZV DNA Qaul RT PCR-SO
Influenza Testing
- Order as Influenza A/B & RSV,RNA by PCR.
- Generally run every 3hrs, starting at 9am,12n,3pm,6pm,9pm. Tests takes 2 hour turnaround.
Chlamydia/Neisseria gonorrhea RNA:
- females - urine or cervical (not vaginal)
- males - urine or urethral
- urine - yellow tube, fluid level in between black lines
- cervical/urethral - white swab to clean mucus, blue swab for specimen collection
- don't use Rectal-SO or Throat-SO orderable unless you are specifically checking these sites
Malaria/Thin Smear
- Order as Blood Parasite Exam
Pathology Tissue Request:
- label prints as soon as the order is signed and cannot easily be printed again.
- printed in MD room on label printer if ordered from computer in MD room
- printed in patient room on label printer if ordered from computer in patient room
Peripheral Smear Exam by Lab: usually ordered by non Heme/Onc provider for review by lab tech
Peripheral Smear for Provider Pickup (Slide Wirght Giemsa): usually ordered in consultation with Heme/Onc for MD to personally review
Specimen Collection Instructions - OVMC Micro Quick Reference Guide
http://myladhs.lacounty.gov/ov/Pathology/Documents/Microbiology%20Specimen%20Collection.pdf
Blood Bank
Massive Transfusion Protocol
- MTP Recommendations:
- 1 unit plasma for every 1 unit PRBCs
- 1 unit of platelets for every 6 unit PRBCs
- Due to necessity of thawing plasma units, plasma will be given when available
- Step 1: Call Blood Bank x74062 to activate MTP
- a. Need Name and MRUN (John Doe name/MRUN from Reg ok)
- b. Need Attending Name
- Step 2: Order “Blood Product Pick Up Slip – MTP” in Cerner
- a. MD or RN can do this
- b. Clerk prints out pick-up slip
- c. No co-sign needed
- Step 3: Send runner to blood bank with printed pick-up slip to retrieve blood
- a. If available, give them:
- Signed Emergency Blood Release Form
- Type and Cross Specimen
- a. If available, give them:
- Step 4: Blood Bank will send up unmatched Type O or type-specific cross matched units with runner
- Step 5: Send Type and Cross specimen STAT if not already sent
- a. MD to order in Cerner
- b. Specimen to be brought directly to Blood Bank
- Need more units?
- a. ALWAYS give them “Blood Product Pick Up Slip”
- b. If not yet sent, give them Signed Emergency Blood Release Form
- Follow-up: Have MD order blood products and transfusion orders for blood products infused
- one blanket order for 6 PRBCs, 6 plasma, 1 platelets, 1 cryo is acceptable. Order can be reconciled later to reflect exact amounts
Pharmacy
- ED Pharmacist Mon-Fri 8am-4pm x75490
Hours
- Monday - Friday 7:30am-8pm; Sat, Sun, Holidays 8:30am-4:30pm
OVMC Empiric Antibiotic Recommendations 2019-2020
Rhogam Administration
- Cerner: RhIG Request, click on both Administer and RhIG Request, then Initiate, then Modify both: Administer Intramuscular and RhIG Request 1 vial and reason Prenatal. Then Orders for Signature and Sign.
Medication Refill Patient Handout
http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Pharmacy%20Refills.pdf
Safe Prescribing and Narcan Handouts
- Safe Prescribing English http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Safe%20Prescribing%20ED%20English.pdf
- Safe Prescribing Spanish
http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Safe%20Prescribing%20ED%20Spanish.pdf
- Narcan (Naloxone) English http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Naloxone%20English.pdf
- Narcan (Naloxone) Spanish http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Naloxone%20Spanish.pdf
Buprenorphine Administraton
- See Substance Use Disorder
Physical Therapy, Occupational Therapy and Orthotics
ED Orthopedic Equipment and Hernia Trusses
- Crutches, walkers, canes – stored in ED1A and ED5 clean utility rooms
- Hard shoes, wrist braces, ankle splints - stored in Orthopedic Storage Room
- Hernia trusses – stored in Room #43
DME Supplies to be ordered as outpatient
- Order supplies such as compression stockings as "DME..."
- Order will ask Diagnosis, length of use, etc. For compression stockings, use 20-30mmHg
- Instruct patient to go to Physical Therapy room 1D120 to pick up the supply
- Do NOT use for OOP patients; please send to health plan.
- Link will take you to list of DME supplies: http://myladhs.lacounty.gov/ov/DEM/Documents/DME%20Supplies.xlsx?Web=1
Urgent Spinal Bracing - TLSO Brace, Miami J Collar, St. Jude Collar etc
- Place order in Cerner: Orthotic Equipment
- Write "TLSO Brace" under Special Instructions
- Call VALLEY INSTITUTE OF PROSTHETICS AND ORTHOTICS (VIPO)
- Cell phone: (661) 319-2777 Mike Nelson, CPO
- Call 24/7 for URGENT spinal bracing otherwise wait until daytime hours
- IPO headquarters: 661-253-1191 or after hours: (800) 439-1005
- VIPO will come to ED with brace or collar if needed before discharge
- Otherwise patient can be sent to our Physical Therapy on T/Th to pickup brace or patient can go to the company headquarters in Santa Clarita
- Cell phone: (661) 319-2777 Mike Nelson, CPO
- If Mike Nelson cannot be reached, the following vendors can be tried (all have DHS contracts):
- PERFORMANCE PROSTHETIC AND ORTHOTIC CENTER, INC (310) 829-2322 LERMAN AND SON (310) 659-2290
- ALPHA ORTHOPEDIC APPLIANCE COMPANY, INC (323) 721-6706
- HANGER PROSTHETICS & ORTHOTICS (562) 233-4481
- DYNAMIC ORTHOTICS & PROSTHETICS, INC (213) 383-9212 ORTHO ENGINEERING, INC. (310) 559-5996
- PRECISION ORTHOTICS & PROSTHETIC, INC. (213) 388-5847
Wheelchairs
- Wheelchairs are kept in the ED for after-hours and weekend patients to avoid admissions, e.g. wheelchair-bound patients or patients requiring wheelchair for example bilateral ankle fractures
- Ask RNs where they are kept; or Use Backup Supply list (top of WikEM) and search where wheelchairs are kept
- Alternative ordering process:
- Order DME in Cerner- Do NOT order on OOP patients - must go to Health Plan for wheelchair
- Order Physical Therapy Outpatient Future Order also in Cerner
- Patient should be sent to Physical Therapy. Patient will be financially screened. If patient has no insurance to pay for wheelchair through DHS, patient/family will be given list of outside vendors to contact.
Physical Therapy and Occupational Therapy Outpatient
- Do NOT send OOP; refer patient to their health plan
- Order as Physical Therapy Outpatient or Occupational Therapy Outpatient Future Order in Cerner
- Patient should be told to go to PT/OT Office, 1st floor, XXXXX. Patient will be financially screened. If patient has no insurance, patient/family will be given list of outside physical therapy centers to contact.
Guidelines
- Physical Therapy
- Post-op or acute shoulder injuries
- Neck, trunk, lower extremities
- Face
- Gait, balance, mobility and transfer training
- Conditioning
- Cardiopulmonary
- Lymphedema
- Chronic Wounds
- Neuro conditions (except upper extremity)
- Occupational Therapy (in general)
- Finger, hand, elbow, wrist injury, fracture, or post-op
- Chronic shoulder issues/pain
- Frozen shoulder
- If patient has difficulty with ADLs, such as bathing, dressing, grooming, feeding
- Neuro conditions that affect the upper extremity
- Fine motor control
Back Pain Classes
- Order as Physical Therapy Outpatient Future Order in Cerner; PT Program: PT Eval and PT Reasons: Back Class as choices in the order
For Emergency Calls After Hours
- You may call Physical Therapy by having OVMC Operator use the Disaster Fan-Out list to reach Physical Therapy. Joann York will be the first one tried, then other staff within the Physical Therapy Dept.
Procedure Clinic
Paracentesis, Thoracentesis, Lumbar Puncture
- Medicine Procedure Service (sponsored by the Department of Medicine, Division of Pulmonary and Critical Care)
- Send requests to OVM Procedure Service ED/UC Urgent Followup Message Pool and patients will be contacted with instructions and scheduled for the requested procedure.
- Patients will check into Outpatient Special Procedures Area on the 2nd floor on day of procedure. (Procedures done in Medicine Procedure Room on 5th floor).
- Ensure patient has good contact phone number in ORCHID. Appointment will be mailed.
- If patient does NOT have reliable phone number, please page Procedure Service Pager 818-313-1733 or x73820 (M-F 8 AM to 4 PM) and we will attempt to give a date/time/instructions.
- If lab tests are needed on the specimen, please request this in Orchid message to Lisa Morgan RN
- Patients will be financially cleared prior to scheduled appt.
- Followup appts for those who need procedures such as paracentesis regularly will be arranged by the Medicine Procedure Service.
Respiratory Therapy
Respiratory Therapy contact phone numbers
- RT supervisor x75038
- RT DEM resp therapist x75581
- RT Lead resp therapist x75331
BiPAP, Transporting patients upstairs on portable BiPAP
- Often we have patients on BiPAP who need to be admitted upstairs.
- RT currently has 3 BiPAP (V60) machines that have a battery backup so patients can be transported upstairs without turning off the BiPAP
- Ideally, before placing a patient on BiPAP, we should tell RT that the patient is likely to be admitted so RT can place the patient on a BiPAP machine that has battery backup.
- If the patient is already on BiPAP that does not have battery backup AND taking the patient off BiPAP would be detrimental to the patient, ask RT about switching the patient to a unit that has battery backup
- If absolutely necessary, RT has the option to rent a BiPAP machine which can generally be here within 30-60mins.
- RT Supervisor Jim Pratt is always available (RT is able to page him) if a question cannot be answered by RT
Home O2, How to obtain
- Call Resp Therapy x74422
- If already on oxygen and has moved to L.A., lost insurance, etc, will need to prove need for home O2. Get pulse ox on room air. Qualifies if O2 Sat less than 88% on room air.
- Resp Therapy will bring a Durable Medical Equipment form that will need to be filled out by the ED provider
- Resp Therapy will contact the company, fax over the form, and arrange for delivery
- O2 TANK CAN BE DELIVERED TO THE ED so patient can leave with O2. More tanks will be arranged to be sent to patient's home
- On occasion, the company may not have O2 tanks readily available in which case patient needs to be admitted to the hospital
- If patient has an outside health plan (OOP), UR may need to be involved for coordination of care
Social Work
Contacting Social Worker
- "Consult to Social Work" in Cerner - will send automatic page to SW and fax to the SW office
- Social Work 7am - 7:30pm pager 818-313-1759
- Social Work 7:30p-7am (off campus) 818-313-1637 for emergencies such as deaths, significant child abuse
- Social Work ED Office 74930
- Social Work 1st floor Office 74236
Sexual Assault
- OVMC does not have an adult Sexual Assault Nurse Examiner (SANE)
- Call police dept in jurisdiction/city where assault occurred
- Police must take patient to our closest center for sexual assaults which is Northridge Hospital
- Northridge Hospital Center for Assault Treatment Services 818-908-8630
Child Maltreatment/Abuse
- See Pediatrics
Transporting patients home
- For patients without ability to get home (e.g. brought in by EMS), and no family or friends to take them home, first option is to have patients wait in waiting room until bus resumes in morning.
- SOCIAL WORKER DOES NOT HAVE BUS TOKENS
- If more urgent transportation is necessary, County Trans can be used on a case-by-case basis to transport patient home. Patient must have a key to house/apartment. County Trans will not transport to shelters.
Translation Services
- In Person Translation Services for Hard of Hearing, Deaf, Deaf Blind, and Non ASL Speakers
- For American Sign Language, Tactile, and Certified Deaf, In-Person Interpreter Services: Please contact Accommodating Ideas at (800)257-1783 M-F 8:00am to 10:00pm; for Weekends, Holidays and after above hours, call Heather C. at (818)481-9028.
- They work with contractors and will aim to provide you with an interpreter as soon as one is available.
- Please have Accommodating Ideas form completed and available when you call:
- Always include your P.O. Number: DO-HO-19034844-1 effective 09/25/18 thru 06/31/19
- Your interpreter must be requested for a minimum of 2 hours
- Our ED clerks will email Accommodating Ideas at aiterps@ai-ada.com & always CC: Laura Onofre, CHI at Lonofre@dhs.lacounty.gov for invoicing purposes and verification
- You may reach Laura Onofre, CHI at (747) 210-3411 M-F 8:00 am to 4:30 pm, for any support or clarification of the process
- For American Sign Language, Tactile, and Certified Deaf, In-Person Interpreter Services: Please contact Accommodating Ideas at (800)257-1783 M-F 8:00am to 10:00pm; for Weekends, Holidays and after above hours, call Heather C. at (818)481-9028.
Olive View Trauma Recovery Center
- We provide mental health and wrap-around case management for victims of crime in the San Fernando and Antelope Valleys.
- Who is eligible for services?
- Anyone who has been a victim of crime in the past 3 years and/or the victim’s family members.
- Has a need for mental health and/or case management.
- Not currently under the care of a mental health professional.
- Anyone who has been a victim of crime in the past 3 years and/or the victim’s family members.
- We aim to serve:
- 1. Crime victims who typically are unable to access traditional services, including, but not limited to, victims who are homeless, chronically mentally ill, of diverse ethnicity, members of immigrant and refugee groups, disabled, who have severe trauma-related symptoms or complex psychological issues, or juvenile victims, including minors who have had contact with the juvenile dependency or justice system.
- 2. Victims of a wide range of crimes, including, but not limited to, victims of sexual assault, domestic violence, physical assault, shooting, stabbing, human trafficking, and vehicular assault, and family members of victims.
- How do I refer a patient?
- 1. From Olive View- In ORCHID, place a social work consult with the reason “Other” and write “Trauma Recovery Center Referral” in the comments.
- 2. From outside Olive View- go to our website https://oliveviewtrc.org/ and use the referral form tab.
- FAQs
- 1. Do you provide services for children? Yes
- 2. What if the crime happened outside the U.S.? We can still provide services to the victim.
- 3. Does the potential client have to be DHS eligible? No, we can provide services regardless of insurance plan or lack thereof.
- Email: olvtrc@dhs.lacounty.gov
- Phone: (747)210-4800
- Web: oliveviewtrc.org
- Social: Instagram – @oliveview_trc
Medico-Legal Resources
Olive View now has a Medical Legal Community Partnership (MLCP) in conjunction with Neighborhood Legal Services. If you have a patient who has legal issues that impact their health (unsafe housing, MediCal issues, immigration, employment, etc) they can now consult with a lawyer on the OV campus through the MLCP. There is a lawyer available by appointment in the social work office on Tuesdays and Thursdays. The way to refer is to put in a social work consult order for the patient with the reason as "other" and in the comments write "request MLCP visit for..." with the reason for the referral. See below flyers for more information about areas where they can help.
Violence Intervention Programs
- https://www.allianceforcommunityempowerment.org/
- https://www.championsinservice.org/
- https://www.lagryd.org/refer
Immigration Resources
The changes to the public charge rule went into effect in February 2020. This has created high levels of fear among our patients because it has the potential to impact future adjustments in immigration status. There is lots of misinformation out there about these changes. For the most part, our patients can continue to obtain healthcare within the DHS without any problem. If a patient has a concern about whether receiving care or signing up for benefits will impact their ability to adjust their immigration status, please give them the attached flyer from the Office of Immigrant Affairs of Los Angeles County. They are available to help answer questions about what these changes mean for specific patients and families. Public Charge Information Card: Link to Info Card
- County Policy on Sensitive Locations: http://myladhs.lacounty.gov/ov/DEM/PublishingImages/SitePages/EMHome/LA%20County%20Sensitive%20Locations%20Policy%20-%20October%2019%202017.pdf Alt Link
- Know your Rights flyer:
- English: http://myladhs.lacounty.gov/ov/DEM/PublishingImages/SitePages/EMHome/Know%20Your%20Rights%20Flyers_English.pdf Alt Link
- Spanish: http://myladhs.lacounty.gov/ov/DEM/PublishingImages/SitePages/EMHome/Know%20Your%20Rights%20Flyers_Spanish.pdf Alt Link
- Chinese: http://myladhs.lacounty.gov/ov/DEM/PublishingImages/SitePages/EMHome/Know%20Your%20Rights%20Flyers_Chinese.pdfAlt Link
- Know your Rights pocket card:
- English: http://myladhs.lacounty.gov/ov/DEM/PublishingImages/SitePages/EMHome/OIA%20Know%20Your%20Rights%20Card%20English.pdfAlt Link
- Spanish: http://myladhs.lacounty.gov/ov/DEM/PublishingImages/SitePages/EMHome/OIA%20Know%20Your%20Rights%20Card%20Spanish.pdfAlt Link
- Chinese: http://myladhs.lacounty.gov/ov/DEM/PublishingImages/SitePages/EMHome/OIA%20Know%20Your%20Rights%20Card%20Chinese.pdfAlt Link
Community Resources
- Anger Management http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Anger%20Mgmt.pdf Alt Link
- Bereavement http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Bereavement.pdf Alt Link
- Community Clinic List http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Community%20clinic%20list%20MHLA.pdf Alt Link
- Community Clinic List Children & Families http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Community%20Clinics%20Children%20Families.pdf Alt Link
- Counseling http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Counseling.pdf Counseling
- Counseling Children and Families http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Counseling%20Children%20and%20Families.pdf Alt Link
- Dental Clinics http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Dental%20Clinics.pdf Alt Link
- Dental Clinic Mid-Valley http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Dental%20Mid-Valley.pdf Alt Link
- Developmental Delay Services http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Development%20Delay%20Services.pdf Alt Link
- Domestic Violence Shelters & Services http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Domestic%20Violence%20Shelters%20Services.pdf
- Drug & Alcohol Referrals I http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Drug%20and%20Alcohol%20I.pdf Alt Link
- Drug & Alcohol Referrals II http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Drug%20and%20Alcohol.pdf Alt Link
- Food Pantry and Clothing http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Food%20Pantry%20and%20Clothing.pdf Alt Link Updated List Feb 2020: [3]
- Heat Relief and Cooling Centers (English) https://ready.lacounty.gov/heat/
- Heat Relief and Cooling Centers (Spanish) https://ready.lacounty.gov/calor/
- Heat Relief and LA's Green New Deal https://plan.lamayor.org/neighborhood-council/neighborhood_council.html
- Homeless Shelters http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/homeless%20shelters.pdf Alt Link
- Legal Services Spanish http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Legal%20Services%20Spanish.pdf Alt Link
- Mental Health Community Resources http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Mental%20Health%20Community%20Resources.pdf Alt Link
- Mental Health Urgent Care http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Mental%20Health%20Urgent%20Care.pdf Alt Link
- Mental Health Perinatal Depression http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Mental%20Health%20Perinatal%20Depression.pdf Alt Link
- Smoking Quitting http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Smoking%20Quitting.pdf Alt Link
- Vision Clinics http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Vision%20Clinics.pdf Alt Link
- Vision Valley Community Clinic http://myladhs.lacounty.gov/ov/Departments/DEM/Forms/Social%20Service%20Resources/Vision%20Valley%20Community.pdf Alt Link
Substance Use Disorders
- OVMC Bridge Website: https://www.ovmcbridge.org/
Substance Abuse Counselors in the ED and SASH Hotline
- Contact Substance Use Disorder Counselor through Consult to Social Work, drop down Substance Use Disorder
- Refer DHS patient to MAT Bridge Message Pool
- SASH Helpline (Substance Abuse Service Helpline) 1-844-804-7500; 24/7; Patient will speak to a counselor who will ask questions and help patient obtain services for detox and rehab
Opioid Use Disorder Recognition and Treatment/Bridge Program
Goal is to recognize opioid use disorder and initiate treatment with buprenorphine or methadone while the patient is in the ED or hospitalized.
- Consult Social Work for ALL Opioid Use Disorder patients even if they do not want treatment
- Consult to Social Work......Substance Abuse.....free text OUD
- V. Figueroa is our Substance Use Coordinator, Mon-Fri, 8am-5pm, 818-792-0407
- Medications for Opioid Use Disorder (MOUD) On-call provider 8am-8pm 7 days per week: 818-313-1451
- Bridge provider on-call can help with recognition of OUD, help with buprenorphine or methadone initiation in the ED and MOUD provider will make sure the patient gets follow-up
- OVM MAT Bridge ED/UC Urgent Follow Up Message Pool to refer DHS patients to Bridge for follow up.
- PLEASE DOUBLE CHECK PATIENT'S CONTACT PHONE NUMBER IN CERNER
- Additional Resources:
- California Poison Control 24/7 access to addiction fellow/attending for help with difficult cases: 844-326-2626
- UCSF Substance Use Warmline, access to help with difficult cases, Monday-Friday 6am-5pm: 855-300-3595
- ovmcbridge.org has a lot of education, videos on a variety of SUD topics
Buprenorphine and Methadone Administration in the ED
- For any patient with opioid use disorder, OD, withdrawal or seeking care, please page the Meds for Opioid Use Disorder provider on-call 8am-8pm 7 days per week, 818-313-1451
- Call Dr. McCollough if unable to reach MOUD provider OR anytime 8pm-8am. 310-614-5306 WE WANT TO KNOW ABOUT ALL OF THESE PATIENTS!
- Please also Consult to Social Work....Substance Use Disorder....OUD in free text
- Viviana Figueroa is the Substance Use Navigator for the Bridge OUD program - 747-210-5625, pager 818-226-4824, Mon-Fri 8am-5pm
- ED initiation of buprenorphine (Bup) for patients with opiate use disorder has been shown to increase likelihood patients will continue with addiction treatment. Bup has been shown to decrease mortality.
- ED Bridge guidelines encourage a higher loading dose of Bup (up to 32mg) which allows patients time to get into an outside addiction treatment program.
- Buprenorphine may be ordered during the ED visit by ED providers without an X-waiver. ED providers without an X-Waiver have may treat a patient up to 72 hours (3 contiguous days) in order to bridge the patient to outpatient treatment. This means the patient must return to the ED if symptoms reoccur. ED providers WITHOUT an X-waiver cannot prescribe.
- If patient really wants methadone instead, that also can be started in the ED. Follow-up will be arranged by our Bridge team as patient must go to a licensed methadone clinic. PLEASE MAKE SURE WE HAVE A CORRECT PHONE NUMBER
- MOUD Providers all have their X-Waiver and can eprescribe buprenorphine to our pharmacy or to an outside pharmacy
- Bridge program (Viviana and staff) will ensure patient gets follow-up PLEASE MAKE SURE WE HAVE A CORRECT PHONE NUMBER.
- OVMC Substance Use Disorder Education and Management Website http://myladhs.lacounty.gov/ov/Substance_Use_Disorder_Management/SitePages/Home.aspx
- ED Bridge Guide https://static1.squarespace.com/static/5adf7f1fa2772cb4f86018b2/t/5aff30cf758d46c1c95b5a40/1526673619420/ED-BRIDGE+BUP+GUIDE+-+MAY+2018+%282%29.pdf
- ED Buprenorphine Initiation Algorithm
- ED Buprenorphine Initiation for Pregnant Patients Algorithm
- ED Buprenorphine Initiation after Overdose
- Buprenorphine and Acute Pain in the ED
- Buprenorphine and Acute Pain on the Med/Surg Unit
- Methadone Quick Start
- Home Start of Buprenorphine Instructions http://myladhs.lacounty.gov/ov/Substance_Use_Disorder_Management/PublishingImages/SitePages/Home/NIH%20Simplified%20Buprenorphine%20Home%20Start.pdf
- CA Bridge website https://www.bridgetotreatment.org/
- Need help?
- California Poison Control 24/7 access to addiction fellow/attending for help with difficult cases: 844-326-2626
- UCSF Substance Use Warmline, access to help with difficult cases, Monday-Friday 6am-5pm: 855-300-3595
- ED Bridge Office Hours https://ed-bridge.org/office-hours
Transfers
MAC phone number 866-940-4401, press 3 for DHS facility
Higher Level of Care Transfers
- Patients who require services that OVMC does not offer may need to be transferred out (e.g. neurosurgery, some emergent orthopedic cases).
- For OOP patients who are clinically stable, every attempt should be made to transfer the patient to their health plan.
- For uninsured or DHS-empaneled patients, transfer will occur through the MAC.
- Transfers from the ED via the MAC fall into two categories. This is based on existing DHS policy:
- (1) Emergent/Urgent e.g. intubated intracranial bleed. MAC will ask minimal questions in order to get transportation to OVMC as quickly as possible. CMO on-call (ask Operator)should be notified regarding emergent transfer. Emergent/Urgent patients cannot be refused by Harbor or USC and may end up being transferred to their ED if no inpatient beds are available. Emergent/Urgent transfers should be used on a rare basis for those patients who need to move RIGHT NOW aka emergently.
- (2) Non-Urgent e.g. open tib/fib fracture or hip fracture. MAC will ask more detailed questions. Patients will be presented to appropriate service at USC or Harbor. Transportation will be arranged after patient has been accepted.
- Remember both USC and Harbor have DHS Cerner and have access to our ED records and imaging
- MAC will NOT transfer to private hospitals such as transfer of neuro patient to UCLA for intracerebral thrombolysis (exception burn cases) or pediatric patient who is followed by UCLA sub specialist at the OVMC clinics. Transportation of those patients must be arranged by the private hospital or OVMC UR.
BLS vs ALS vs Critical Care vs Helicopters
- BLS is staffed by EMTs, limited abilities, can administer oxygen; cannot push meds and cannot have any hanging IV drips
- ALS is staffed by paramedics, can take intubated patients, CANNOT take patients with ANY type of IV drip (no heparin, mannitol, norepi, etc) even if those drips are not titratable. Drips must be shut off. ALS IS ABLE take maintenance IV with max of KCl 20meq/L. ETA variable.
- Critical care is staffed by paramedics plus Critical Care RN and/or MD, can take intubated patients with IV drips. Often ETA of critical care team arrival 4-5 hours away.
- Helicopter is staffed by paramedics +/- critical care RN, can take intubated patients with IV drips. Dependent upon weather. ETA variable.
- For critically ill or injured patients on a drip that cannot be turned off, if critical care team's ETA is too long, consider sending OVMC ED RN, MD and/or RT as needed in ambulance. Arrange head of time for same ambulance to bring staff back to OVMC.
Pediatrics
- The Pediatric attending on-call should be made aware of any higher level of care transfer out
- For OOP pediatric patients, UR should attempt to transfer the patient to the hospital requested by the health plan
- For uninsured patients, not currently followed by a pediatric sub-specialist, attempts should be made to transfer to USC or Harbor via the MAC
- Patients followed by UCLA Pediatric subspecialties at OVMC may be transferred to UCLA if accepted by UCLA Pediatrics or subspecialist.
- OVMC Pediatric resident will contact UCLA inpatient staff or subspecialty service about transfer with approval by the Pediatric attending on-call
- Once accepted, transportation will depend upon the type of transfer: PICU transfers may transported by the UCLA Transport team; Ward transfers to UCLA will need to have transportation arranged by OVMC ED UR staff.
- MAC WILL NOT ARRANGE TRANSPORTATION TO UCLA
Surgical and surgical subspecialties
- For all surgical and surgical subspecialties being transferred out for "higher level of care", please contact the Attending of that service prior to transfer out. ED Attending should speak to Surgical Attending to ensure we do not have the ability to care for the patient here at OVMC
Neurosurgery
- See Neurosurgery
Utilization Review (Utilization Management)
- x74890
- Outpatient Service Coordinator OPSC can help with urgent follow-up to primary care for OOP patients (see above Follow-Up...Out of Plan OOP)
ED Ultrasound
Link to OVMC Ultrasound website
Transvaginal Ultrasound
ED Supplies and Equipment
Tutorial Videos
- Compass® disposable Pressure Monitor for Lumbar punctures https://www.youtube.com/watch?v=Fzcd7ef7N3U
- Compass® disposable Pressure Monitor for Central Venous Pressure (CVP): https://www.youtube.com/watch?v=1zLpLXY5W6E
- Compass® disposable Pressure Monitor for Compartment Pressures: https://vimeo.com/117488817
Clerk ED1A Cabinet
- Alligator Forceps
- Bolt Cutter
- Doppler
- Dremel
- EZ-IO
- Hair Remover
- Panoptic
- Ring Cutter https://www.youtube.com/watch?v=VGE8oYtyR6k&feature=youtu.be
- Rongeur
- Stryker https://wikem.org/wiki/Compartment_pressure_measurement
- Tonopen
*MUST LEAVE BADGE FOR ANY EQUIPMENT REMOVED FROM CLERK CABINET
ED1A MD Room
- Ultrasound Supplies
- Gel
- Probe covers
- Angiocaths 3inch
- Headlamp
Airway Cart in PR Room
- CO2 detectors, ETT
- CO2 detectors, nasal
- Nasal Atomizers
- Trach Atomizers
- Endotracheal Tubes
- LMAs
Room 31
- Upper Cabinet
- Nosebleed Trays
- Lollicaine Lollipops (lidocaine lollipops)
- Ophtho Micoscope
- Cable for Xenon lamp
- Magnifying Headlamp
- ENT Cart
- OPHTHO
- pH paper taped to pH folder on top of cart
- OROPHARYNGEAL
- NASAL
- Nasal compression device for nose bleeds
- Nasal speculum
- Merocel
- Surgicel 2" x 3"
- Silver nitrate sticks
- Rhino Rocket Slimline - small, medium, large
- Rapid Rhino 5.5cm Rapid Pac
- Rapid Rhino 7.5cm Ant/Posterior with Airway
- Vaseline Petroleum Gauze Strip 1" x 36"
- Denver Nasal Splint
- Wood's Lamp bottom drawer
- OPHTHO
Suture Cart
Ortho Cart
Gyn Cart
Central Line Cart in ED 1A/B hallway
Orthopedic supplies in Room 43
- Soft collars, slings, wrist guards, CAM walkers, hard shoes
- Abdominal binders
- Hernia truss
Crutches, Walkers, Wheelchairs
- Located in ED1A/B Clean Utility Room
Bronchoscope
- Located in storage room near Triage 4. Disposable scopes in cabinet in same room.
Glidescope
- Located in PR Room - pediatric and adult batons available
- Disposable blades located in Glidescope basket
- Extra blades located in cabinets in PR Room
- Wipe down batons after each use
Unusual Supplies
- Gastrostomy Tubes - ED 1A MD Room "S**T HAPPENS" Cabinet
- Nephrostomy tubing and bags - try OR
- Whitacre Spinal Needles - LP Cart
- Merlin Pacemaker Interrogator - ED 1A Cabinet
- This device interrogates pacers and ICDs made by St. Jude or Abbott. The detailed instructions are printed and posted inside of the cabinet door and included below. It requires cellular data transmission. First interrogate the patient's device at the bedside, then move the unit to the ambulance bay and plug it in there so it can transmit. The report is subsequently faxed to the ED1 nursing station and is also transmitted to the device reps and our cardiology service. The device reps are on call for assistance as needed, or you can call Scott Lundberg to try and help.
Disaster Preparedness
- Olive View-UCLA has a robust plan for a number of possible disasters such as earthquakes. All OVMC faculty and residents should review the materials on the hospital homepage under “Disaster Management.” The link is in the center of the screen. For staff in the ED at the time of a disaster, the important information is as follows.
- 1. The ANO (Acting Nursing Officer) is designated as the incident commander and is in the hospital 24/7.
- 2. The ANO will set up a command post in Hospital Administration and will contact the charge nurses in each department.
- 3. The initial priority is a head count of all staff, and a report on the physical condition of the department.
- 4. A physician in the hospital will be designated as a medical officer in the incident command center. At night, this may be OB or Anesthesia as they are also in house and we will be responsible for managing the ED.
- 5. All requests for materials, staff, and questions go though the incident command in medical administration.
- 6. The ED charge nurse is aware of the location of extra supplies and the hospital wide disaster management plan.
- Olive View-UCLA has over one week of food, water and medical supplies for an anticipated disaster. There are specific incident commanders and disaster professionals who will be responding, and the emergency physicians on site are not expected to lead the disaster response.
Downtime Protocols
Downtime Documentation
- H&P will be documented on paper using DEM Physician Record (OV1901). Resident and Attending signatures are required.
- MSE - when performed by a separate MSE provider, note should be very brief and be written on the upper portion of the History section of the paper DEM Physician Record (OV1901). It should include a separate header of MSE NOTE and must be signed.
Downtime General Orders
- orders should be written on paper using DEM Physician’s Orders (OV1337) and include a date, time, initials, and signature
- orders should be placed in the order bin located at each Nursing Station (ED 1-5, RME) for the Nurse/Clerk to initiate
- clerk has all downtime forms, lab slips and Radiology Request forms.
Downtime Radiology Orders
- order imaging on paper and include a complete paper Radiology Order Form (OV2059). Runner will hand deliver request to the appropriate ED radiology area.
- if ORCHID downtime is isolated, iimages and preliminary results will still be available in Synapse even if not viewable in ORCHID
- radiology orders ordered during downtime using the Radiology Request forms do NOT routinely need to be re-entered into ORCHID after ORCHID comes back up (exceptions may occur).
Downtime Laboratory Orders/Workflow
- clerk/nurse will complete paper lab request slips to accompany specimens sent to the lab. The lab slip should include collector's employee number ("e" or "c" number).
- lab labels will not print during downtime. All specimens must be labeled with the following information:
- patient info: patient name, DOB, MRN, FIN
- collector's info: date/time specimen collected, employee number ("e' or "c" number), collectors signature
- lab results will be faxed to the ED at X74298 and hand delivered to the assigned resident or attending for that patient
- POCT orders placed by the providers will be resulted verbally to the ordering provider and also resulted in nursing documentation
- lab will call critical results to the ED
- lab orders ordered during downtime do NOT routinely need to be re-entered into ORCHID after ORCHID comes back up (exceptions may occur). Results that came back on paper will eventually also be resulted in ORCHID.
Downtime Medication Orders
- all medication orders should be written on paper using form OV1337
- patient prescriptions should be written on paper and handed to the patient. A copy of each Rx should be kept in the patient’s paper record. Rxs will be scanned into ORCHID once ORCHID comes back up. Rx’s will not be back entered by the provider into ORCHID after a prolonged downtime.
- when ORCHID is back up, Pharmacy will manually enter all medications that were ordered during downtime
Downtime Blood Bank Orders
- enter required orders on paper (T&S, T&C, transfusion, etc)
- paper blood transfusion indication sheet must be filled out for Adults OV1998 or Peds (OV2015)
Downtime Specialty Diagnostic Services
- complete paper requisition for Echo, Stress Treadmill/Myocardial Perfusion Imaging, Holter and EEG. Call appropriate department for STAT orders
Downtime Admissions
- initiate Interqual request by calling UR directly at X74890.
- discuss with admitting team
- once an admission is accepted by the admitting team, enter Request to Admit order on paper and include service, level of care, and the name of the admitting attending and resident.
- admissions during downtime will be tracked by Nursing on a paper log
- certain orders such as Bed Requests and Admit Orders will need to be manually re-entered into ORCHID once ORCHID is back up
Downtime Discharge
- complete discharge and aftercare instructions using form OV2014 including discharge impression, recommended follow up, and return precuations. Do not use this form for Rx.
- Rx should be written on paper Rx pads. Copies should be left in paper chart to be scanned in later.
- discharge order must be signed on paper
- all discharges from the ED during downtime will be tracked by Nursing on a paper log. A separate provider log will be kept for downtime discharges that require future labs, studies, message pools, e-consults, TFU referrals so that they may be entered into ORCHID during recovery.
Downtime Recovery - ORCHID Back Online
- LAB/RAD - results will begin to populate via the interface in ORCHID. Lab and imaging orders previously placed on paper should not neeed to be ordered again.
- documentation – Provider documentation on paper will be scanned into patient chart.
- pharmacy will back-enter enter all medication orders placed on paper during downtime back into ORCHID.
- physicians must re-enter all other paper orders placed during downtime into ORCHID (admission requests, place in obs, isolation, communication, restraints, holds, consults, etc).
Downtime Frequent Phone Numbers
- ED Lab (8:30 am - 10:30pm) : 74977
- General Lab: 73476, 74038
- Microbiology: 76041
- Blood Bank: 74062
- Phlebotomy: 74555/74039
- ED Xray Tech: 75496
- ED US Tech: 74940
- ED CT Tech: 74968
- MRI Tech: 73535
- ED Radiologist: 74971
- StatRad Coverage for CT and MRI Overnight and Weekend Reads Only - 858-546-3800, press 1.
- USROC Coverage for Ultrasound Overnight and Weekend Reads OnlyMonday-Friday 11p-7a and Weekends/Holidays 7p-7a 866-448-7762
- ED UR/Interqual: 74890
- Pharmacy: 73070
- ED1A: 74320
- ED1B: 74865
- ED2A: 74321
- ED2B: 74280
- ED3: 74976
- ED4: 74974
- ED5: 74970
- SuperTrack Provider Room : 74936/74937
- Main Provider Room: 73645
- DEM Administrative Offices: 73107
ORCHID/FirstNet
Logon
- logon credentials are the same as your Internet Password
- if you need to reset your password go to the Olive View- UCLA Home Page, under the Links Section (toward the bottom), and choose one of the Password and Account Management links
- if you still can’t logon, call the Enterprise Help Desk at x74522
CheckIn
- at the start of a new shift, ORCHID should immediately prompt you to check-in as an available provider.
- in the Provider CheckIn window, select your Display Name, Provider Role and a Default Relation. Also select the checkboxes for Available Provider and Available Reviewer.
- if you were already checked-in to see patients on that shift, you will not be prompted to check in again.
- if you need to Check In manually, click on the little icon of the provider with the Check Box.
Patient Sign Up
- click once on the patient row then click on the Assign Provider icon. Your Display Name will appear in the appropriate column.
Documentation
Selecting a Note Template
- click Provider Notes from the tracking list then +Add in the Provider Notes band
- the Note Type should default to ED Note-Provider so that notes are filed in the correct folder and can be viewed by UR and the ED Attending once they are saved. If the ED Note-Provider option is not available, right-click on the arrow to select from All Note Types.
- using the Reason For Visit tab select a Note Template to use either by free text search or by using the structured menu (PNED RFV) then hit select OK. Use the checkboxes to select which elements (if any) you would like to import into your note
- colored notepads on the Tracking Board track the progress of your Provider Note (not started, in progress, or signed) during the patient encounter
Documentation Workflow
- once saved, notes written using the default ED Note-Provider template, can be viewed by both Utilization Management and the ED Attending. Consultants cannot view provider ED documentation until the note is signed.
- once you have completed your provider note, click on Sign/Submit and a new window will pop up. Select Request Endorsement, then click inside the yellow area under Endorser. Select the binoculars icon to search for the attending you would like to co-sign your chart. Click OK. Under “Type” make sure that sign is selected (not reviewed). Then click sign to close the window.
- Attendings: In the Message Center you can view notes forwarded to you for signature. Choose the Correct icon to change a note and write an addendum. If you want to write a separate note before the intern/resident has completed their note, use the Note function (rather than Provider Notes).
- for patients signed out at rounds, the oncoming resident should write a brief note using the Notes function (not Provider Notes).
Documenting a Re-Evaluation
- below the Medical Decision Making section of the PowerNote note there is a section to document follow up exams. Choose Re-exam/Re-eval and enter a time before entering details of the follow up exam
- right-clicking over the Re-exam/Re-eval header and selecting repeat allows you to document repeated re-evaluations
Getting Rid of Spellcheck
- Open a patient's chart and start a note
- Click View at the top.....then Customize.....then More......unclick Run Spelling check....click OK
Unable to place Diagnosis?
- Usually because HLI: Physician Friendly Term box has not been checked
- Step 1: Type in desired diagnosis and click Binoculars
- Step 2: Click the 3 dots just to the right of "Terminology"
- Step 3: Check the box HLI: Physician Friendly Term
- Step 4: You may have to close the Diagnosis box and re-enter the diagnosis
Procedure Consent with iMedConsent
- iMedConsent is now accessed directly through Cerner from within a patient's chart. There is an iMedConsent tab available under the Table of Contents Menu (Table of Contents are the grey tabs on the left hand side of the mPage underneath the "ED Summary"). Users no longer have to manually enter patient identifiers to search for a patient. There is no longer a need to maintain a separate username and password for iMedConsent.
- select the appropriate procedure/s that you would like to print for the patient
- have the patient read, consent, and wet sign the printed procedure consent form
- place a copy of the wet signed consent in the patient's paper chart. The Health Information Management (HIM) team will scan the consent form into ORCHID after the patient is discharged.
Procedure Documentation (ad hoc forms)
- AdHoc Forms are used for specific template driven documentation in the ED. This includes documentation of all ED Procedures. AdHoc forms can be found using the AdHoc link on the ORCHID Menubar,
then finding the ED Forms Folder.
- template AdHoc forms include documentation for ED Procedures, ED Bedside Ultrasounds, Central Line (CLIP) documentation, and the NIH Stroke Scale.
- once completed, these AdHoc forms are signed using the Check Mark on the Upper Left corner of the screen.
Medicine Admissions
1) Interqual Request Order - found on the Quick Orders page under the Top Other section. A diagnosis is required.
- DHS uses Interqual Criteria for Utilization Review (UR). All admissions must be reviewed by UR. The Interqual decision is facilitated by having a note in the chart for UR to review. UR can view ED resident notes as long as they have been saved.
- the Interqual Request is found under the Events tab and the Request Events sub-tab.
- the Interqual review process is tracked with ICONs under the ADT column
- REQ - Requested
- IP - In Progress
- MET - Criteria Met the
2) Contact the admitting team via Amion to give report
- contact the admitting Hospitalist or Resident. Use auto-paging (see below) to help track the time the admitting service is first paged. Confirm with the Hospitalist the name of the receiving Attending, Resident, Service, and Level of Care
3) Enter the Request for Admit. Enter the admitting resident name in the Special Instructions field. Medicine teams will drop Admission orders in the chart within 2 hours from the time the Request for Admit order is placed.
- Note: Admission orders should NOT be placed on any patient until Bed Control updates their location status to ED Boarders. ED Boarders are easily identifiedin the location field on the Banner Bar and by a slash in the Bed
column on the FirstNet track. If inpatient orders are dropped on a patient before they are changed to an ED Boarder they will have to be re-entered by the Admitting team.
- the Hospital Icon indicates that the inpatient team has placed Admitting Orders in ORCHID. The Medicine team assumes all responsibility for patient care once Admission orders are placed. Routing questions from Nursing regarding further medical care should be directed to the inpatient provider.
Changes in Service or Level of Care after Initial Admission
- if you need to upgrade/downgrade an ED Boarder after the initial Request for Admit has been submitted, you need to order Request for Admit again (not Transfer). This is the only way bed control will get the message that a change has been requested. DEM providers will do this if they are still following the patient, however once Admission Orders are written (Hospital Icon), the Admitting Service will re-order the Request for Admit if any upgrade/downgrade must occur.
- if the post-admission upgrade/downgrade results in the patient going to a different team, the Inpatient team must notify and give report to the new team since these patients are no longer being followed by the ED.
Surgery Admissions
- the process is similar to the Medicine admission process with the following exceptions:
- the Request for Admit order is held until the admitting team evaluates the patient in the ED
- the ED resident places the the Request for Admit order once the admitting information is confirmed with the surgery team
- Note: the surgery team should NOT place Admission orders in ORCHID until the Request for Admit is placed and the patient’s location has been updated to an ED Boarder otherwise orders may have to be re-written when the patient goes upstairs
ED Holding Orders
- if the inpatient team has already accepted a patient, but there is an unavoidable delay (> 2 hrs.) in placing admission orders, the ED Team can initiate the ED Holding Orders Order Set for the inpatient setting to either facilitate boarding care in the ED or to facilitate transportation to an available bed upstairs. Make certain the inpatient team is contacted so they are aware ED Holding Orders have been initiated and that the patient may go upstairs.
- as with all admissions, do not place ED Holding Orders unless the patient has already entered ED Boarding status (see Med Admissions above).
Observation Patients
- the observation unit is used for patients who require additional care after the ED but less than 24 hours of hospital care. The decision to place a patient in the OBS unit should be made in conjunction with the ED Attending and Hospitalist
- observation patients do not require Interqual
- once the patient has been accepted by the Hospitalist for OBS status, order Place in Observation from the ED Quick Order page (top other section)
- patients should NEVER be placed in OBS status after a Request for Admit has been ordered
Consultation & Auto Paging
Consults - No Auto Paging OVMC
- consult initiation time can easily be documented by placing the consult order from the Other Pane on the lower right side of the Adult ED Quick Orders page.
- once the Consult order is signed, a marker is placed on the Events tab. Hovering over this marker will show the duration since the consult was first placed. When the consult is complete, this can be documented by right- clicking over the active order and completing the consult. Once complete it will be removed from the Tracking List.
Consults - Auto Paging OVMC
- a selected number of consults also page the provider automatically when the consult is placed. In these Orders, the Call Back Phone Number is the only required field. The provider receiving the page will NOT see any instructions included in the Special Instructions on their pager but these instructions can still be reviewed on the Review Orders pane.
- clear pages from the list using the red X Icon under Task
- Note: DO NOT click on the close window button to close the ED Paging error will result. Instead use the Minimize window Icon.
ECGs
Triage ECGs
- nurse will bring paper Triage ECG to the Attending for review
- ED attending will verbally tell the nurse what to do (STEMI, BRING BACK, or TRIAGE)
- paper EKG stays with Attending as a reminder to document their read in FirstNet ECG Viewing/Documentation
- on the FirstNet track, under the ECG column, double click on the completed EKG ICON
- in the ECG Review Pane, free text either the Triage ECG read (i.e. STEMI, BRING BACK, or TRIAGE), or a more comprehensive read (follow up ECGs)
- save the ED read by selecting “ED Review & Close” into the window then hit ED Review and Close.
- the EKG Icon will now have a checkbox on it
- once EKGs are visible in Cerner and have a ED preliminary read documented, they can be shredded
Viewing Prior ECGs
- all ECGs from the current FirstNet encounter are accessible directly from the ECG column
- ECGs from previous ORCHID encounters are available in the Flowsheet tab under the the Cardiology View and Cardiovascular CV Filters
- ECG archives prior to ORCHID are accessible in Tracemaster using the patient’s legacy Affinity MRN. It can be accessed either through Wellsoft or Clinical Workstation.
Entering ED Provider Radiology Wet Reads
- from the Tracking List, right-click on the Rad column of any completed imaging order and the Order Info window will open. Click the blue +Add button to display the Wet Read window.
- select Positive or Negative and free text your wet read then enter OK
- a red exclamation icon indicates a wet read has already been entered. Click the exclamation mark to view or add another wet read
- wet reads may also be entered from the Radiology Results section of a Power Note by using the Launch Wet Read button.
Medical Students in FirstNet
Documentation
- refer to the Documentation section for detailed documentation instructions.
- initiate and save a note (without signing) early during a patient encounter after taking a history and performing your exam. Next, present to the Attending physician.
- update your note with any follow up including medical decision making, lab/imaging results, and/or patient updates.
- once your note is finalized, hit Sign. A window will pop to “Request Endorsement” of your supervising attending to endorse your note. This request will show up in their Message Center.
- Attendings: medical student notes forwarded to you will show up in your Message Center in a preliminary status. Once reviewed, a brief note documenting supervision should be added, then the note should be signed.
- students who leave the ED must sign out all their patients to either an NP or resident after reviewing the overall plan with their supervising attending.
Order Entry
- after discussing with the Attending, enter proposed orders into ORCHID. Medical students cannot use Quick Orders.
- access the Modular Order Entry Window by going to the Menu pane and select +Add from the Review Orders band.
- enter the name of the Attending you will be proposing orders to for co- signature.
- search for orders individually and enter all required details
- these orders will be forwarded to the attending once you sign them but they won’t become active until co-signed by the Attending. To speed up turn around time, remind the attending verbally that orders are in their Message Center and ready for co-signature.
Order Entry
Quick Orders
- from the Tracking Board choose a patient then select Place Orders to go to the Quick Orders page
- orders can be added to the green ‘Shopping Cart’ by selecting them off your menu of choice or via the search line in the New Order Entry widget
• once order selection is completed, click on the green shopping cart to sign, save, modify, or cancel all of the selected orders. If additional required details are required you will be prompted to enter them • orders can also be entered using the Modular Order Entry Window which is accessed by hitting +Add from the Review Orders menu pane
Required Order Fields
- many orders in ORCHID cannot be signed without filling out required fields. During order selection on the order pane, required fields are indicated by a blue circle icon with an “X”. Within order details, required fields are indicated with a yellow background, bold-face lettering, or an asterisk
- use the Missed Required Details button to rapidly cycle through a long list of orders with required details
- alternately, multiple orders can be selected together (SHIFT-select) or (CTRL-select) and common fields shared among them can be addressed more easily
Copying Orders
- if you would like to repeat an order, right-click on an active order and select Copy. It will be available for you to sign again.
Discontinuing Orders
- to discontinue any order, right-click on the active order and select Cancel/Discontinue. Note: Don’t forget to sign after you discontinue an order!
Lab Orders
Collection Priorities
- Add – to add another test to a sample that is already in the lab. Prior to ordering a test with the Add priority, you must first verbally confirm with the lab that they can run this test with an existing sample.
- Stat – all ED labs
- Timed Stat – used when the same STAT test is ordered and a Frequency id included (i.e. Troponin q6h). Enter a duration (i.e. 3 times) so that the order will not continue indefinitely. If a Frequency is added to a Stat priority ORCHID will automatically change the Collection Priority to Timed Stat
Nurse Collect:
- “No”: most ED labs should be ordered as Nurse Collect “No.” The lab order is tasked directly to the phlebotomist. Nurses can intercept the order and draw it themselves if desired.
- “Yes”: the lab order is specifically tasked to the bedside nurse. If the phlebotomist is available, the nurse can call phlebotomy to perform the draw.
- Note: lab orders should never need to be re-ordered simply due to the incorrect selection of the Nurse Collect field.
Order Sets
Order Sets
- Order Sets are individual orders grouped together to simplify order entry for common indications or procedures. Commonly used Order Sets for the ED can be found on the Quick Orders page, under the Order Sets widget. One may also search for Order Sets using the prefix “ED” on any Order search field.
- all Order Sets are designated by a yellow Icon with multiple geometric shapes. They are designed with some individual orders being pre-selected, however each included order can be selected, modified (right-click) or un-selected prior to order signature
Adding Orders from an Order Set already Initiated
- Searching/launching an Order Set repeatedly is usually not necessary. If you need to go back into an active Order Set and add or modify something, you can do so without having to reorder the entire Order Set. Go to the Review
Orders menu, highlight the Order Set under the Plans section of the Order View pane, then click the light bulb icon called “View Excluded Components.” Orders already active will show up indented and checked, and all unordered components will have empty boxes. Select the orders you would like to add or discontinue then sign.
Discontinuing Order Sets
- to discontinue an Order Set, find the active Order Set in the Order View pane and then right-click to select Discontinue.
- you will be given the option of choosing which orders to Keep active even though the rest of the Order Set is being discontinued.
- Note: Don’t forget to sign after you discontinue an Order Set!
Order Favorites
Order Favorites
- right-click on any order before signature and select Add to Favorites
Lab Results
- hover over the lab column to rapidly view what lab tests have been ordered. The Lab Indicator column on the track shows how many labs have been ordered and how many labs are resulted. Double-click on the Lab Indicator to see a detailed view (Quick View) of lab results. To see full lab results in details click on the Vitals/Nursing/Results pane
Imaging Results
- hover over the lab column to rapidly view what lab tests have been ordered. The Rad Indicator column on the track shows how many imaging tests have been ordered, how many have images available, and how many images have a preliminary read in ORCHID.
- double-click on the Rad Indicator to open the Quick Flowsheet Radiology tab.
- click on the Result box to open up the Document Viewer to view the read if available.
- viewing Images: within the Document Viewer, click on the image icon to open a link to Synapse and view the image from within ORCHID. You may have to enter your login credentials to open Synapse.
Discharge & Follow Up
Discharge Process
- select patient from the Tracking List then hit the Admit/Discharge button
- open each pane by clicking on the pencil
- fill out the required and optional fields as needed. The Check Marks will help keep track of your progress.
- Diagnosis, Prescriptions, Med Reconciliation
- Patient Education - education handouts and Work Excuse notes
- Follow Up Date - to communicate follow up with your patient. Note: This does NOT result in actually scheduling appointments!
- ED Post Visit Plan - TFU/CCC referrals (see below)
- ED NERF - new NERF referrals (see below)
- Note: DO NOT SELECT THE DISCHARGE PANE! This is how the nurse removes the patient from the Tracking List.
Follow Up
- once fully registered, patients who cannot follow up at Olive View should have an Outside Of Plan Icon in their Events column. These patients should be referred elsewhere.
Message Pools
- only for Urgent Appointment requests to selected clinics, that need to be seen within 2 wks. Many of these clinics previously used the “wallbox" referral system.
- select a patient on the Tracking List then select Communicate - > Message. Patient Name should Autofill.
- TO: Binoculars Icon, Pool filter, search for the correct Message Pool (see list), Add to Send to list, hit OK.
- Subject: choose OVM ED/Urgent Care Appt Request from the menu
- fill out template, check Patient Needs Appointment box, and Send
TFU/CCC Clinics
- part of the Depart Process. Open the ED Post Visit Plan band and Route to either the Telephone Follow Up Clinic (ED-TFU-OVM) or the Continuity Clinic (ED-CCC- OVM). Specify need for referral and Contact Phone number
- Click on the Check Mark at the Upper left to close this window.
eConsult
- the eConsult referral system should be used for non-urgent outpatient referrals that can wait more than 2 weeks to be processed. eConsults should be entered by the Attending Physician using the eConsult link on the ORCHID menu bar.
ED NERF
- patients new to the county that qualify for outpatient primary care (no OOP Icon) can be referred to primary care using the ED NERF tab. Choose as many diagnoses that apply then click on the Check
- Mark at the Upper Left of the referral window.
Ordering Outpatient Studies (Future Orders)
- once a patient is sent home from the ED, all pending orders are automatically cancelled unless they are entered as Future Orders. Any labs, tests, or referrals to be completed after ED discharge should be entered as Orders for Future Visit. This includes all outpatient imaging and cardiology tests.
- Physical Therapy: outpatient PT should be ordered using Physical Therapy Evaluation and Treatment Outpatient as a future order.
- Outpatient FNA: outpatient FNAs should be processed as an eConsult by the Attending Physician. The eConsult destination specialty is Pathology - Fine Needle Aspiration. Patients can then show up directly to the lab during regular business hours.
Patient Portal (LA Health Portal) / Giving Medical Records to Patients


LA Health Portal QR


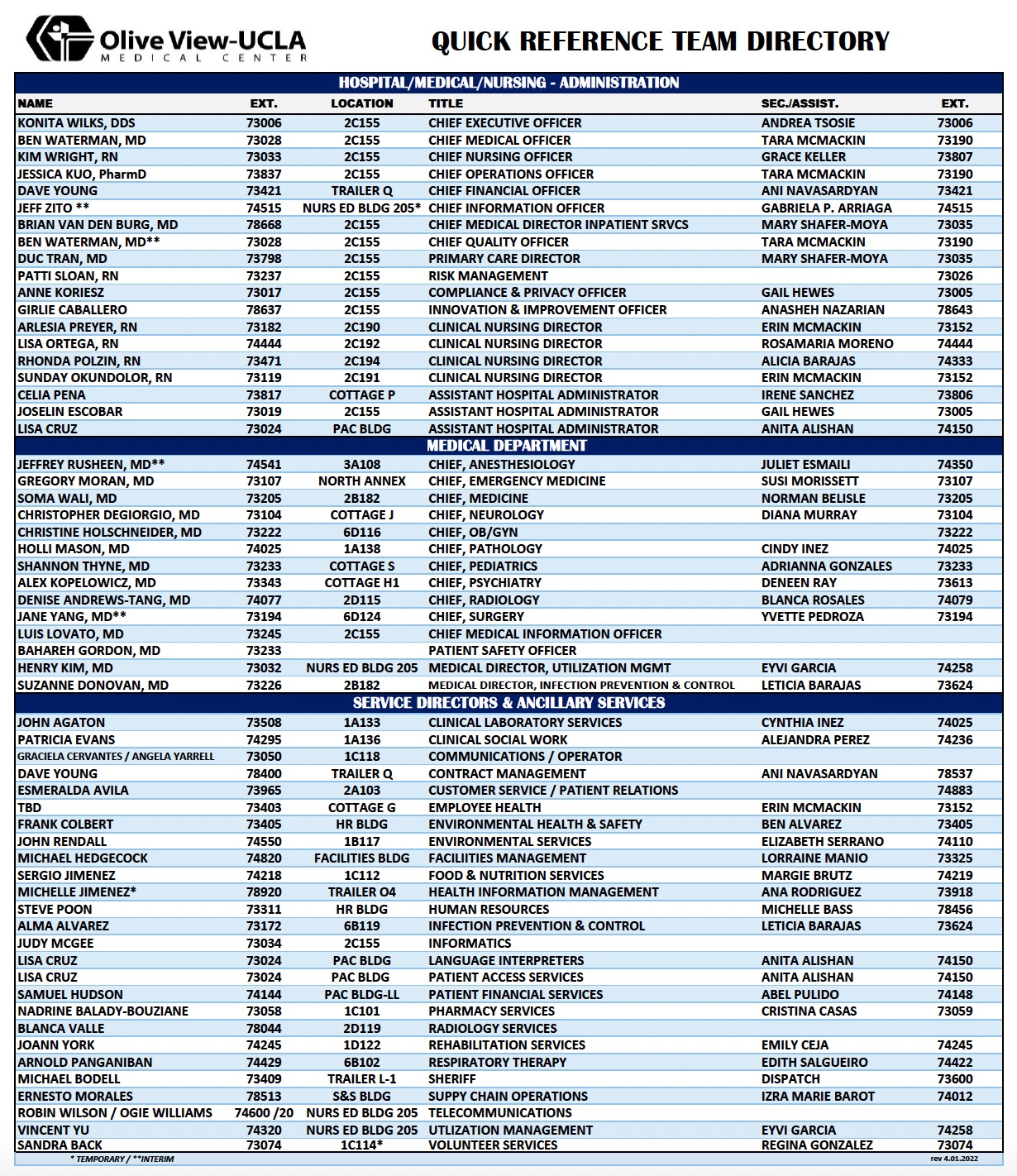{kind=link}
The LADHS Health Portal is an extremely important resource to give our ED patients so they may access their own medical records. This includes labs, imaging, provider notes, and ED discharge instructions. This is the best way to give our "OOP" patients access to records they need to share with outside providers. Patients can access the LA Health Portal via the web or by using the LA Health Portal smartphone app (iOs and Android App Stores).
Enroll Patient in Portal
See widely distributed recruitment fliers in ED with QR code for patient smartphones. Best workflow is for patient's to use their own smartphones. All the patient needs to enroll is their name, birthdate, and medical record number (preferred) to confirm who they are. An email or text phone number can also be used to confirm who they are, but only if the email or text number is already in their registration information in ORCHID.
Alternately patient can use any WOW to enroll, but will likely need assistance in finding the LADHS Health Portal website.
Nursing staff are also encouraging LA Health Portal Enrollment for all of our patients.
ED Registration staff can assist if phone numbers or email addresses need to be updated, but neither is required for a new enrollment.
During regular business hours, the OVMC Health Tech Navigator, Jennifer Vargas, can also assist with complicated Patient Portal enrollments (reset existing passwords, proxy access, etc). Jennifer Vargas x74546 - jvargas4@dhs.lacounty.gov
Procedure References
These links should serve as a reference for safe and proper techniques on how to perform many common (and some uncommon) procedures in the ED. For some procedures there may be both a longer video explaining in-depth details if this is your first time (eg med students and interns) and a shorter video if it's been a while and you just want to brush up.
Basics
Lumbar Puncture:
- NEJM (10:59) https://www.nejm.org/doi/full/10.1056/NEJMvcm054952
- Mellick (3:14) https://www.youtube.com/watch?v=grpeEDBMrn8
Paracentesis:
Resuscitation
IO line Placement
- EMRAP (3:12) https://www.youtube.com/watch?v=KHXSfh2ZRDM
US-guided IV Placement
- 5 Min Sono (5:52) https://www.youtube.com/watch?v=4Znd21vJPb8
Central Venous Catheterization
- NEJM (15:28) https://www.nejm.org/doi/full/10.1056/NEJMvcm055053
ENT
Facial Nerve Blocks
- Inferior Alveolar Nerve Block: FreeDentalEducation (4:48; procedure at 2:15) https://www.youtube.com/watch?v=kmPqV-dMo98
- Infraorbital Nerve Block: Brian Lin (2:00) https://www.youtube.com/watch?v=3nzXe_NYKlg
- Mental Nerve Block: The Dental Box (1:06) https://www.youtube.com/watch?v=hPALXAq9pTo
Nasal Foreign Body Removal
- BVM for Complete Occlusion: Robert Dudas (0:51) https://www.youtube.com/watch?v=PacvHiJFhNA
- Katz Extractor for Partial Occlusion: Larry Mellick (3:22) https://www.youtube.com/watch?v=rQpIOdJrYIc
GI
Balloon Tamponade
- Minnesota: EMRAP (5:08) https://www.youtube.com/watch?v=4FHIiA_doWU
- Blakemore: EMRAP (4:47) https://www.youtube.com/watch?v=NHelCd5Jtp4
Digits
Digital Block
- CORE EM (2:34) https://www.youtube.com/watch?v=i51y6t1YRNQ
Paronychia
- Brian Lin (3:35) https://www.youtube.com/watch?v=G9CBKoKEvRM
Subungual Hematoma Drainage
- EMRAP (1:02) https://www.youtube.com/watch?v=G_7eKSYLfxY
Rongeurs
- EMRAP (2:30) https://www.youtube.com/watch?v=zBmsrGzPk40
Links
- http://www.amion.com
- http://www.emergencymedicine.ucla.edu
- http://www.uclaemultrasound.org
- OVMC FirstNet Training Website