Background
- Cyanotic
- Acyanotic
- Differentiation by pulmonary vascularity on CXR[1]
- Increased pulmonary vascularity
- Decreased pulmonary vascularity
Clinical Features
| Clinical Presentation
|
Causative Conditions in Neonates
|
Causative Conditions in Infants and Children
|
| Cyanosis |
Transposition of the great arteries, TOF, tricuspid atresia, truncus arteriosus, total anomalous pulmonary venous return |
TOF, Eisenmenger complex
|
| Cardiovascular shock |
Critical aortic stenosis, coarctation of the aorta, HLHS |
Coarctation of the aorta (infants)
|
| Congestive heart failure |
Rare: PDA, HLHS |
PDA, VSD, ASD, atrioventricular canal
|
| Murmur |
PDA, valvular defects (AS, PS) |
VSD, ASD, PDA, outflow obstructions, valvular defects (AS, PS)
|
| Syncope |
— |
AS, PS, Eisenmenger complex
|
| Hypertension |
— |
Coarctation of the aorta
|
| Arrhythmias |
— |
ASD, Ebstein anomaly, postsurgical complication after repair of congenital heart defect
|
Differential Diagnosis
THE MISFITS [2]
Evaluation
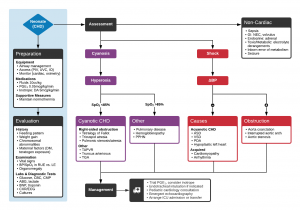
Algorithm for the Evaluation and Management of Suspected Congenital Heart Disease in Neonates
Cyanotic
| Cardiac Lesion
|
Chest Radiograph
|
ECG
|
| Tetralogy of Fallot |
Boot-shaped heart, normal-sized heart, decreased pulmonary vascular markings |
Right axis deviation, right ventricular hypertrophy
|
| Transposition of the great arteries |
Egg-shaped heart, narrow mediastinum, increased pulmonary vascular marking |
Right axis deviation, right ventricular hypertrophy
|
| Total anomalous pulmonary venous return |
Snowman sign, significant cardiomegaly, increased pulmonary vascular markings |
Right axis deviation, right ventricular hypertrophy, right atrial enlargement
|
| Tricuspid atresia |
Heart of normal to slightly increased size, decreased pulmonary vascular markings |
Superior QRS axis with right atrial hypertrophy, left atrial hypertrophy, left ventricular hypertrophy
|
| Truncus arteriosus |
Cardiomegaly, increased pulmonary vascular markings |
Biventricular hypertrophy
|
- Can use the "5 T's' mnemonic:[3]
- 1 vessel: Truncus arteriosus
- 2 vessels switched: Transposition of the great vessels
- 3=TRIcuspid: Tricuspid atresia
- 4 defects: Tetralogy of Fallot
- 5 letters: Total anomalous pulmonary vascular return (TAPVR)
Acyanotic (duct-dependent)
| Coarctation of the aorta
|
Cardiomegaly with pulmonary edema (neonate)
|
RVH, right bundle-branch block (neonate)
|
|
Rib notching and collateral vascularity (child) |
LVH (child)
|
| Hypoplastic left heart syndrome |
Cardiomegaly |
Right atrial enlargement, RVH, peaked P waves
|
| Aortic stenosis |
Cardiomegaly |
LVH in severe cases
|
Acyanotic non-duct dependent (i.e. CHF)
| Atrial septal defect
|
Cardiomegaly with increased vascular markings
|
Right axis deviation, RVH, RBBB
|
| VSD |
Cardiomegaly with increased vascular markings |
LAH, LVH, (RVH with larger VSDs)
|
| PDA |
Cardiomegaly with increased vascular markings |
LVH, RVH with larger PDAs
|
| Endocardial cushion defect |
Cardiomegaly with increased vascular markings |
Superior QRS axis with RVH, RBBB, LVH, prolonged PR interval
|
| Anomalous origin of the left coronary artery |
Cardiomegaly |
Abnormally deep and wide Q waves with precordial ST segment changes
|
Management
Shock (duct-dependent lesion)
- Knee chest position
- Increased venous return to heart, increased SVR (decreased R>L shunting)
- O2
- Morphine or NS to increase preload
- Sodium bicarbonate 2mEq/kg IV bolus (promotes vasodilation)
- Propranolol 0.2mg/kg IV (relieves infundibular spasm)
- Phenylephrine 2-10mcg/kg/min to increased SVR
Thrombolysis for Surgical Shunt Obstruction
- Blalock-Taussig shunt should maintain flow murmur
- Loss of flow murmur alongside profound hypoxia relative to baseline saturations should prompt consideration for shunt obstruction
- Definitive treatment is surgical, but systemic recombinant tPA may be considered as salvage intervention when other options are not readily available[4]
- Heparin bolus 50-100 u/kg
- Notify cardiology, CT surgeon, ECMO
- 0.01 mg/kg bolus r-tPA, then 0.03 - 0.06 mg/kg/hr
Disposition
Medication Dosing
Prostaglandin E1 0.1mcg/kg/min IV/IO IV/IO
Propranolol 0.2mg/kg IV IV
Phenylephrine 2-10mcg/kg/min IV infusion IV
See Also
References
- ↑ Knipe K et al. Cyanotic congenital heart diseases. Radiopaedia. http://radiopaedia.org/articles/cyanotic-congenital-heart-disease
- ↑ Brousseau T, Sharieff GQ. Newborn emergencies: the first 30 days of life. Pediatr Clin North Am. 2006 Feb;53(1):69-84, vi.
- ↑ Waldman JD, Wernly JA. Cyanotic congenital heart disease with decreased pulmonary blood flow in children. Pediatr Clin North Am. 1999;46(2):385-404. doi:10.1016/s0031-3955(05)70125-5
- ↑ Diaz F et al. Systemic thrombolysis with recombinant tissue plasminogen activator for acute life-threatening Blalock-Taussig shunt obstruction. Indian J Crit Care Med. 2016 Jul; 20(7): 425–427.
