Background
Ankle stabilization anatomy
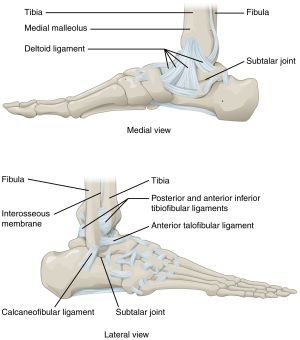
Ligaments of ankle and feet.
- Syndesmosis
- Ligaments
- Medial: Medial collateral (deltoid) ligament (tibia to talus and calcaneus)
- Lateral: Anterior/posterior talofibular, calcaneofibular ligaments
Clinical Features

Right foot with acute lateral ankle sprain.
Lateral Ankle Sprain
- Most common
- Due to inversion of plantarflexed ankle
- Anterior talofibular ligament (ATFL) is most commonly injured ligament
Medial Ankle Sprain
- Isolated sprain is unusual; often associated with fibular fracture or syndesmosis injury
- Always rule-out Maisonneuve fracture by evaluating proximal fibula
Syndesmotic Sprain ("High-ankle sprain")
- Associated with with hyperdorsiflexion when talus moves superiorly and separates tibia/fibula
- Pain just above talus
Differential Diagnosis
Evaluation
- Anterior drawer test
- Tests anterior talofibular ligament
- Cup heel with one hand and and pull anteriorly while pushing tibia posteriorly
- Talar tilt test
- Tests for combined injury of anterior talofibular and calcaneofibular ligaments
- Inversion at the ankle causes tilting/lifting of the mortise joint
Imaging
Ankle x-ray needed if:
- Pain near the maleoli AND
- Inability to bear weight immediately and in the ED (4 steps) OR
- Tenderness at posterior edge or tip of lateral malleolus OR
- Tenderness at posterior edge or tip of medial malleolus
Foot x-ray series needed if:
- Pain in the midfoot AND
- Inability to bear weight both immediately and in the ED (4 steps) OR
- Tenderness at the navicular OR
- Tenderness at the base of the 5th metatarsal
Exceptions
- Age <6 or >55
- Only for blunt trauma mechanism
- Does not apply to subacute/chronic injuries
- Does not apply to injuries of the hindfoot or forefoot
Classification
- Grade I
- No tearing of ligaments
- Minimal pain, swelling, ecchymosis; weightbearing is tolerable
- No splinting/casting; weight bearing as tolerated, isometric exercises, full ROM and stretching/strengthening exercises
- Grade II
- Partial ligament tear; possible instability
- Increased pain, swelling, ecchymosis; difficulty bearing weight
- Immobilize with air splint; PT with ROM/stretching/strengthening exercises
- Grade III
- Complete ligament tear; significant instability
- Severe pain, swelling, ecchymosis; inability to bear weight
- Immobilization and possible surgery; PT same as grade 2 but longer time period
Management
- Stable joint and ability to bear weight: (Likely Grade I)
- NSAIDs, RICE (rest, ice, compression, elevation)
- 1 week follow up if no improvement
- Stable joint but unable to bear weight or unstable joint (Grades II and III) :
- Ankle cast immobilization or a removable walking boot for 7-10 days for grades II and III. Follow up at 5 days with ortho/podiatry. [1]
- Posterior mold splint and ortho consult/referral
Disposition
Calculators
Ottawa Ankle Rules
Ottawa Ankle Rule
| Criteria
|
No (0)
|
Yes (+1)
|
| Ankle X-ray is required if there is pain in the malleolar zone AND any of the following:
|
|
| Bone tenderness along distal 6 cm of posterior edge of tibia or tip of medial malleolus
|
1
|
|
| Bone tenderness along distal 6 cm of posterior edge of fibula or tip of lateral malleolus
|
1
|
|
| Inability to bear weight both immediately and in the ED (4 steps)
|
1
|
|
| Foot X-ray is required if there is pain in the midfoot zone AND any of the following:
|
|
| Bone tenderness at the base of the 5th metatarsal
|
1
|
|
| Bone tenderness at the navicular
|
1
|
|
| Inability to bear weight both immediately and in the ED (4 steps)
|
1
|
|
| Positive Criteria
|
/ 6
|
| Interpretation
|
| Score = 0
|
No X-ray needed — Sensitivity 96.4–99.6% for clinically significant fractures.
|
| Score ≥ 1
|
X-ray recommended — Ankle and/or foot x-ray indicated based on positive criteria location.
|
| References
|
- Stiell IG et al. A study to develop clinical decision rules for radiography in acute ankle injuries. Ann Emerg Med. 1992;21:384-390. PMID 1554175.
- Stiell IG et al. Decision rules for radiography in acute ankle injuries: refinement and prospective validation. JAMA. 1993;269:1127-1132. PMID 8433468.
|
See Also
References



